 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 93-96 Original Article Thoracic outlet syndrome: Presentation and management Singh Devender, Pingala RK, Reddy LRC, Vani PVNLS Department of Vascular and Endovascular Surgery, Nizam's Institute of Medical Sciences, Hyderabad Code Number: is06024 Abstract Background : Thoracic outlet syndrome (TOS) is the most confusing and controversial subject; its treatment continues to be a dilemma. The symptoms are due to the neurovascular compression at the thoracic outlet.Aims : The objective of the study was to review our experience with this problem with particular reference to its presentation and management. Settings and Design: A retrospective analysis. Materials and Methods : Seventy-two patients (age range 15-55 years), treated for neurovascular complications of TOS from 1991 to 2005. Evaluation included clinical and radiological examinations comprising of radiograph, color duplex and angiogram with positional maneuvers. Result : Nineteen patients had features of neurogenic TOS, whereas 52 patients presented with arterial TOS. One case was found to have venous TOS. The diagnosis was based on the characteristic history and positive provocative tests. Cervical ribs were seen in 58 cases. Angiogram was performed in all arterial TOS. Conservative treatment offered 74% (14) good results in neurogenic cases. Scalenectomy with cervical rib excision via supraclavicular approach, with or without vascular reconstruction, was done in 46 cases. There was no major complication and 90% (42) cases showed good results. Conclusion : TOS is not an uncommon disorder and often goes undiagnosed. Conservative treatment plays a vital role in neurogenic TOS. In our experience, scalenectomy with cervical rib excision via supraclavicular approach gives good and lasting results with an acceptable outcome and minimum morbidity. Keywords: Cervical rib, scalenectomy, stress test, thoracic outlet syndrome The clinical problem now referred to as thoracic outlet syndrome (TOS) has undoubtedly afflicted mankind since ages. The first reported case of TOS appeared in ′GENESIS′ chapter 22.[1] Huang Ti Nei Ching Sun Wen (the yellow emperor′s classics of the internal medicine, 3000 BC) suggested, ′the inner pulses of the arms denote the state of the adjacent regions; they denote the state of the short ribs.′ The symptomatology was first described by Sir Astley Cooper in 1821. In 1905 John B. Murphy of Chicago showed a connection between cervical rib and subclavian aneurysm.[2] In 1920 Law described ligaments and other structures originating in soft tissues associated with TOS, while in 1927 Adson and Coffey emphasized the role of the scalene anticus muscle in TOS. Oschsner, Gage and DeBakey in 1935 named it the scalenus anticus syndrome and made the first successful resection of the anterior scalene muscle. This syndrome was labeled as ′thoracic outlet syndrome′ (TOS) by PEET in 1956.[3] The syndrome is characterized by symptoms of neurovascular compression at the thoracic outlet and occurs within the population in a spectrum ranging from mild numbness and tingling of the fingers when the arms are placed in certain stress positions to severe functional disability and incapacitation, venous hypertension and arterial insufficiency, sometimes leading to digital gangrene.[4] The diagnosis is based on the characteristic history and a positive stress test. The stress tests commonly performed are hyperabduction, ADSON,[5] costoclavicular maneuver or EAST.[4] Plain radiograph shows the presence of cervical ribs, which is the culprit in over half the cases. Nerve conduction studies are often abnormal in neurogenic TOS.[6] Color Doppler and digital subtraction angiography are helpful for arterial TOS. Most of the patients of neurogenic TOS are benefited by conservative treatment.[3] Severe persistent symptoms necessitate surgery. Early decompression, with or without reconstruction, is considered for arterial TOS to prevent limb loss.[7] Several operative measures have been tried via different approaches.[8],[9],[10],[11] Scalenectomy with excision of cervical ribs along with or without elongated transverse process (if any) via supraclavicular approach widely decompresses the thoracic outlet with an acceptable outcome, minimum morbidity and long-lasting results. This retrospective study presents our experience in the management of TOS. Objective To study the clinical presentations and their management in the patients admitted with TOS
Materials and Methods The records of all patients admitted to the vascular services of the Nizam′s Institute of Medical Sciences, Hyderabad, with thoracic outlet syndrome during the last 14 years (from 1991 to 2005) were called from the medical record department. Seventy-two records were found and analyzed for their presentation and treatment outcome by the author and coauthors. Forty were males and 32 were females (age ranged from 15 to 55 years, with mean age of 30 years). The duration of symptoms was from 1 week to 2 years. Most common symptomatology was claudication and arm weakness. Absent pulses, pulsatile mass and bruit were also the features of many patients. Diagnostic evaluation included a clinico-radiological assessment. After proper history and clinical examination, all the patients underwent provocative stress tests. In addition to palpation of pulses and auscultation for bruits at neutral, adduction, abduction-external rotation and specific provocative positions in patients of arterial TOS, they were subjected to segmental pressure study of the upper limb with photoplethysmography (PPG) of the digits. Color duplex and contrast angiography was mandatory in all patients of arterial TOS (in neutral position and with positioning maneuvers). All the patients of neurogenic TOS were evaluated neurologically and nerve conduction velocity tests were asked for in few patients. Patients with neurogenic TOS were consulted with orthopedic surgeon, neurosurgeon and neurologist to rule out non-TOS conditions. Chest and cervical spine radiographs were obtained to define the presence of a bony abnormality such as a cervical rib, anomalous first rib or healed clavicular fracture. MRI was done in those cases where there was a suspicion of cervical disc lesion. Following patients were excluded from the study:
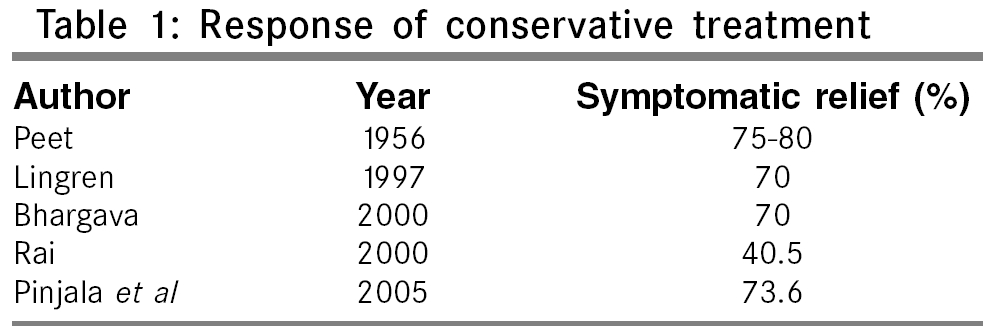
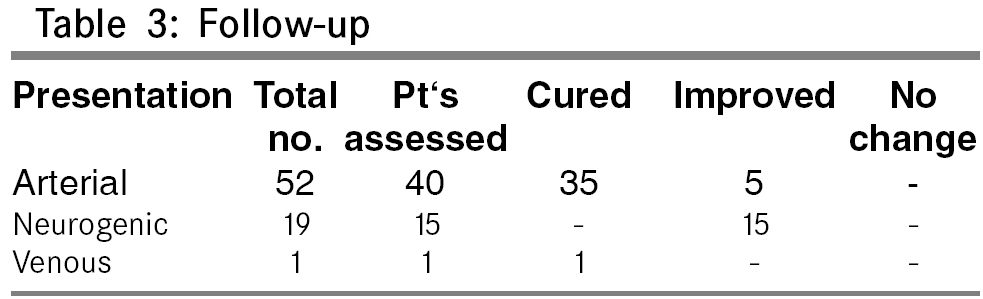
Once the diagnosis of TOS was established with reasonable certainty, patients with neurological symptoms were begun on a program of physical therapy, muscle relaxant, NSAIDs, SWD (short wave diathermy) and narcotics, as needed, at least for 6 weeks. For patients with arterial TOS and for those patients where conservative treatment failed, neurogenic-type surgery was offered. Scalenectomy with cervical rib excision via supraclavicular approach was the principal surgery, associated with other ancillary procedures like claviculectomy, dorsal sympathectomy, thrombectomy and arterial reconstruction with vein or PTFE graft, as needed, in some cases. The patient with venous thrombosis was given anticoagulation and was managed conservatively. After surgery, patients were continued on a regimen of NSAIDs, muscle relaxant and narcotics. Postoperative results were graded as excellent, good, fair and poor according to the following criteria: Excellent - complete relief of symptoms During follow-up, each patient was assessed clinically for reoccurrence of signs and symptoms of TOS and the functional status of the limb was recorded. Objective assessment of the surgical decompression and arterial reconstruction was carried out by means of segmental blood pressure study, PPG and color duplex. Results More than 90% of our patients were under 50 years of age. This study showed a slight preponderance for males; this may be probably due to the less attendance of females in our outpatient department due to social reasons. Nineteen patients had neurogenic TOS presentation with pain, weakness or wasting of small muscles of hand. Fifty-two patients presented with pain, coolness, pallor, Raynaud′s phenomenon. Out of this, 20 patients had limb-threatening ischemia. There was a single patient of venous TOS, who presented with acute thrombosis of subclavian and axillary veins. EAST was the most common positive stress test in about 67% of patients. Radiographs demonstrated cervical ribs in 58 cases (bilateral in 15 and unilateral in 43 cases). A supraclavicular bruit was present in 30 cases. Nerve conduction test was done in 10 cases and an abnormality in ulnar nerve sensory conduction was present in 5 cases. Duplex scan showed subclavian artery stenosis with post-stenotic dilatation in 30 cases, axillary and brachial artery thrombosis in 19 cases and axillary along with brachial vein thrombosis in 1 patient. Seventy-four percent cases of neurogenic TOS were relieved of symptoms with conservative treatment. Five patients of neurogenic TOS and 41 of arterial TOS underwent surgical procedure. Principle surgery of scalenectomy with cervical rib excision via supraclavicular approach was done in all. Thirty patients underwent arterial reconstruction, where end-to-end anastomosis was done in 15 patients, vein graft was used in 8 patients and PTFE graft in 7 patients. Nineteen patients had thrombectomies and in another 9 patients, axillo-distal bypass was done. In other ancillary/associated procedures, 8 patients had claviculectomy, 12 patients had dorsal sympathectomy and 2 patients required digital amputation. Brachial roots were adherent to surrounding structures in 3 patients where neurolysis was performed. The average operating time was 2-4 h. The blood loss was less than 300 ml and none of them required any transfusion. There was no mortality. The average hospital stay was 7 days. There was no major postoperative complication; in the minor complications, 6 patients had wound infections, 3 had hematoma and 9 patients had transient paresthesia. Four patients had Horner′s syndrome, whereas recurrence of neurogenic symptoms were seen in 2 patients who were managed conservatively. Follow-up of 18 to 24 months revealed an excellent response in 67% and a good result in 27% according to the criteria that we followed. The group of patients with vascular TOS did much better than the neurogenic TOS. All the vascular TOS patients had an excellent result after surgery compared to only 50% of the neurogenic TOS patients. Patient with venous occlusion had complete relief of symptoms. On follow-up of patients with arterial TOS, there have been no reoccurrences of arterial symptoms.Discussion The resolution of symptoms of TOS was first achieved surgically by excision of a cervical rib[18] and subsequently by excision of the first rib.[19] Controversies exist as to which technique is better at relieving symptoms of the cervical rib. The incidence of cervical rib is 0.5 to 1% and cervical ribs are thought to cause symptoms in 2 to 35% of affected individuals.[4] In most of the large series, neurological symptoms were responsible for 95% of cases, venous symptoms for 1 to 5% and arterial symptoms for 0.5 to 2%. Like the South Hampton vascular surgical group[21] and Manchester vascular surgical group,[20] we had a preponderance of cases due to vessel compression, which may simply reflect the referral bias to a vascular unit. All the patients with neurogenic complaints were primarily treated with physical therapy. The primary goals of physical therapy are to open up the space between the clavical and first rib, improve posture, strengthen the shoulder girdle and loosen the neck muscles. This is accomplished by pectoralis stretching; strengthening muscles between shoulder blades; assumption of good posture; and active neck exercises, including chin tuck, flexion, rotation, lateral bending and circumduction. Most of our patients were benefited by this and fewer patients required surgical decompression [Table - 1]. Patients with vascular symptoms infrequently had a cervical rib.[14] Most of the patients have been followed up for a minimum of 18 to 24 months. This is especially relevant when looking at the outcome, as it has been suggested that the mean time to recurrence of symptoms is 4 months, with 63% of recurrences occurring within 6 months. The effectiveness of treatment with improvement of over 90% of cases is comparable with other series [Table - 2]. Both Manchester and South Hampton groups suggested that cervical rib alone is probably inadequate for the treatment of patients with vascular symptoms. All patients with vascular symptoms treated by first rib excision by the latter group had a degree of improvement. Of the present patients with vascular involvement, all who had scalenectomy with cervical rib excision showed good improvement [Table - 3]. Other ancillary procedures like thrombectomy, arterial reconstruction, dorsal sympathectomy have their own significance and should be considered whenever needed. In the present series, most of the early complications were like infection and transient parasthesia and only two patients had recurrence of neurological symptoms. These figures are comparable with those in other major series.[10],[14],[15],[17] The worldwide reoperation rate is 1 to 15%, which we did not see in our series.[16] So in conclusion, proper history and clinical examination to diagnose and assess the functional disability are essential. Radiographs, duplex scan and angiogram are important in planning the treatment. In our opinion, when there are only neurological symptoms, it is worthwhile considering the conservative measures for 4 to 6 weeks; and when there is arterial occlusion, reconstruction has a significant role to play. Lastly in our experience, scalenectomy with cervical rib excision via supraclavicular approach gives good and lasting results with an acceptable outcome and minimum morbidity. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06024t3.jpg] [is06024t2.jpg] [is06024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}