 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
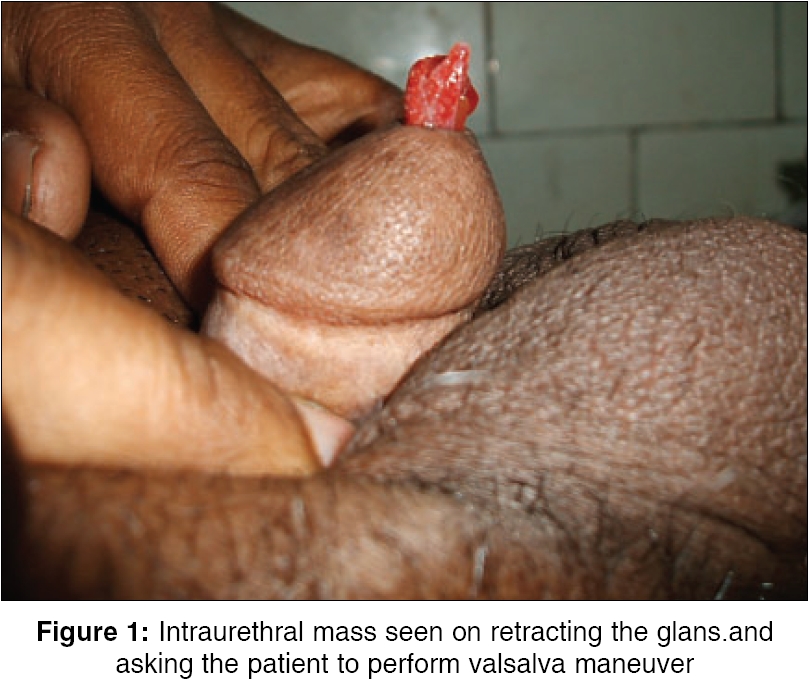
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 97-98 Case Report Recurrent rhinosporidiosis of male urethra Pal DilipKumar, Bhattacharyya N, Bag AK, Sinha L Depatments of Urology, Medical College and Hospital, Kolkata - 73 Code Number: is06025 Abstract Rhinosporidiosis is a chronic granulomatous disease caused by a fungus, Rhinisporidium seeberi . Though the favored site is the nasal mucosa, urethral involvement does occur in this disease, only a few cases are reported in the literature and they are mostly from India. Here we report a case of recurrent urethral rhinosporidiosis, presenting as a protruding mass from the urethral orifice during voiding.Keywords: Male urethra, rhinosporidiosis, recurrent. Rhinosporidiosis is a chronic granulomatous disease caused by a fungus, Rhinisporidium seeberi. Urethral involvement in this disease is very rare, only few cases are reported in the literature and they are mostly from India.[1] The lesion usually presents as a pedunculated or sessile mass involving mainly the nasal mucosa followed by conjunctiva.[2],[3] Other rare sites of involvement are nasopharynx, maxillary antrum, tracheobronchial tree, larynx, skin, vagina, vulva and rectum.[3],[4],[5] Here we report a case of recurrent urethral rhinosporidiosis, presenting as a protruding mass from the urethral orifice during voiding. Case Report A 27-year old man from a rural background, presented with something coming down through the external urethral meatus during voiding, with poor urinary flow and occasional bleeding from the urethra for the last 2 years. He had a similar history before 7 years, for which a protruding urethral mass was excised by a general practitioner, but all the operative records were lost. On examination, he had normal external genitalia with a reddish 1.5 cm long mass coming out through the normal urethral opening, on retracting the glans and asking the patient to perform Valsalva maneuver [Figure - 1]. His hematological and renal biochemical parameters were normal. Color Doppler ultrasonography of the penis showed a highly vascular sessile mass arising from the ventral surface of the urethra, 3 cm proximal to the meatus. Cystourethroscopy suggested a long pinkish mass (3 cm x 1 cm) arising from the ventral surface, proximal to the fossa navicularis with the normal rest of the urethra. Transurethral resection of the mass was done using low coagulation current, with a diagnosis of anterior urethral polyp. Histopathology suggested a nonspecific chronic infiltration of plasma cells and lymphocytes encircling sporangia in different stages of maturity, enclosed in a double chitinous cell wall, leading to a diagnosis of rhinosporidiosis. Follow up cystoscopy at 3 months and one year showed that there was no recurrence or stricture formation at the resection site.Discussion Rhinosporidiosis of urethra is very uncommon and practically unknown in western countries.[1] The lesion mainly occurs in the terminal urethra and sometimes, extensive involvement of the glans can mimic a penile malignancy.[1] The disease mainly affects the younger age group and mostly males.[2],[3],[4] Though it has been reported in two female patients, in a large series of urethral rhinosporidiosis, their spouses were free from the disease.[4] Although the exact mode of contamination is controversial, most of the workers believe that contaminated stagnant water and soil is the source of infection.[3],[4][5] Some are of opinion that trauma to the mucosa is an essential precondition for contamination.[2] Though the disease has a benign course and remains localized, two fatal cases with disseminated rhinosporidiosis have been reported.[4] Surgical extirpation, followed by electro coagulation of the base is the preferred method of treatment.[2],[3],[4],[5] Recurrence has been documented up to 25% due to inadequate resection, as in the present case, or in case of reinfection.[5] Sometimes, partial amputation of the penis may be required, due to extensive involvement of the glans.[1]References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06025f1.jpg] |
| |||||||||

{kind=link}