 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
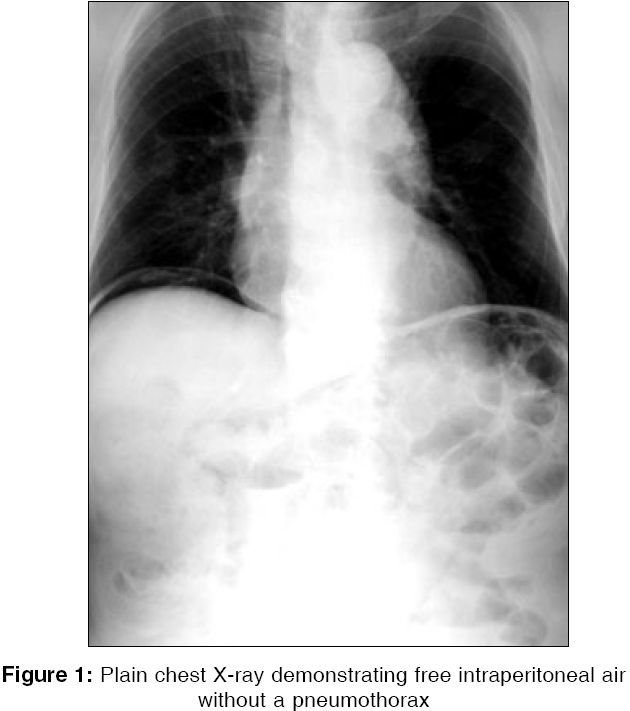
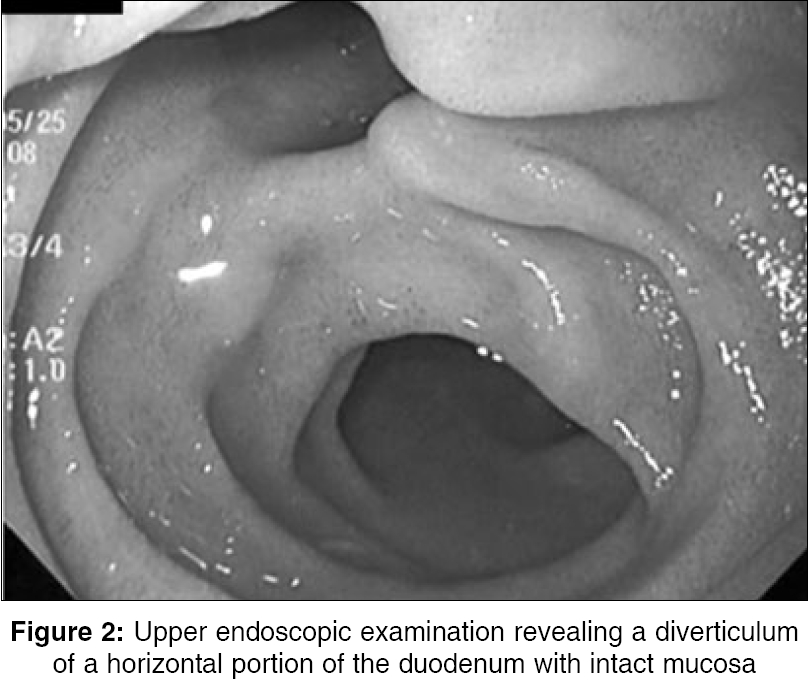
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 99-101 Case Report Asymptomatic spontaneous pneumoperitoneum complicating duodenal diverticulum Hirano Yasumitsu, Hara T, Nozawa H, Nakada K, Oyama K, Hada M, Takagi T, Hirano M Department of Surgery, Kouseiren Takaoka hospital 5-10, Eiraku-cho, Takaoka, 933-8555 Code Number: is06026 Abstract A 91-year-old man was diagnosed with a spontaneous pneumoperitoneum. His abdomen was soft and flat and abdominal examination revealed no tenderness or rebound tenderness. Blood examination did not show signs of inflammation. A chest X-ray demonstrated a pneumoperitoneum without pneumothorax, or pneumomediastinum. Computed tomography showed intraperitoneal free air around the liver, without any other findings. Contrast examination and endoscopy of the upper gastrointestinal tract revealed a diverticulum of a horizontal portion of the duodenum. Spontaneous pneumoperitoneum was diagnosed as being of duodenal diverticulum origin. Conservative therapy including fasting and resuscitation was initiated. Disappearance of the intraperitoneal free air was confirmed 7 days after admission. He was in good health with no clinical evidence of recurrent disease after that. This conservative treatment should be the first choice for management in patients with pneumoperitoneum, in whom a perforated hollow viscus has been excluded by adequate examination.Keywords: Spontaneous pneumoperitoneum, duodenal diverticulum, asymptomatic In over 90% of patients, the presence of intraperitoneal free air occurs after a perforated hollow viscus and these patients usually undergo emergency laparotomy.[1] However, there is a subset of patients in whom no identifiable perforation is found at surgery.[2] Most of them are asymptomatic and have relapsed conservatively.[3],[4],[5] This is called spontaneous pneumoperitoneum. We report herein a case of a 91-year-old man with asymptomatic spontaneous pneumoperitoneum complicating duodenal diverticulum, that was successfully treated conservatively. Case Report A 91-year-old man presented to another hospital for hypertension. Chest X-rays performed for a routine checkup showed free air below the diaphragmatic dome. He was transferred to our hospital for close examination of the pneumoperitoneum on May 21, 2004. His abdomen was soft and flat and abdominal examination revealed no tenderness or rebound tenderness. The remainder of the physical examination was unremarkable. Blood examination showed slight anemia (Hemoglobin 11.9 g/dl) without leukocytosis (white blood cell count 4,400/mm 3) and C reactive protein (CRP) level was not elevated (0.05 mg/dl). A chest X-ray demonstrated a pneumoperitoneum without pneumothorax or pneumomediastinum [Figure - 1]. An abdominal X-ray showed no signs of pnuematosis cystoides intestinalis or small bowel obstruction. Computed tomography (CT) of the abdomen showed intraperitoneal free air around the liver without any other findings. Conservative therapy including fasting and resuscitation was instituted, because there are no findings to suggest peritonitis. Contrast examination of the upper gastrointestinal tract performed 3 days after admission using Gastrografin showed no extravasation of contrast material and revealed only a diverticulum of a horizontal portion of the duodenum. An upper endoscopic examination carried out on the following day showed no pathological findings, except for a diverticulum of a horizontal portion of the duodenum and the mucosa of the diverticulum was intact [Figure - 2]. After endoscopy, abdominal X-ray showed no increase in abdominal air. Spontaneous pneumoperitoneum was suspected as being of duodenal diverticulum origin, because no other apparent findings were detected in closed examinations. Oral administration of nutrition was restarted, but he had no clinical findings of peritonitis afterward. Disappearance of intraperitoneal free air was determined by CT and he was discharged 7 days after admission. The patient has remained in good health with no clinical evidence of recurrent disease, since then.Discussion Pneumoperitoneum seems to be synonymous with perforated hollow viscus and is accompanied by peritonitis. The most common causes of pneumoperitoneum are perforated gastric or duodenal ulcers, perforation of the appendix, or diverticulum of the colon.[6] Most patients with spontaneous pneumoperitoneum continue to undergo emergency laparotomy, because surgeons are taught throughout their training, that free diaphragmatic air mandates emergency surgery. However, about 10% of patients with an unusual cause of pneumoperitoneum, relapse without surgical treatment and this is called spontaneous pneumoperitoneum.[3],[4],[5] In elderly patients, the topic of whether or not surgical treatment should be performed in cases of highly suspected diseases with no definite symptoms, is under debate. This is because the operation itself may worsen the general status, or spoil the quality of life of elderly patients. The various causes of non-surgical spontaneous pneumoperitoneum have been reviewed[3],[7],[8] and they include intra-abdominal causes, such as pnuematosis cystoides intestinalis, jejunal diverticulum and recent abdominal surgery; intrathoracic causes such as pneumothorax, pneumomediastinum, pulmonary disease (pneumonia, bullous emphysema, asthma, etc), trauma, mechanical ventilation and cardiopulmonary resuscitation; gynecologic causes, such as pelvic examination, knee-chest exercises, oral-genital insufflation and vaginal douching; Iatrogenic causes such as laparpscopy, endoscopy and peritoneal dialysis; and miscellaneous causes such as tonsillectomy, aerophasia and dental extraction. According to Medline, there are only three reported cases of spontaneous pneumoperitoneum complicating duodenal diverticulum.[5],[9],[10] A summary of them is given in [Table - 1]. Conservative treatment was selected in three patients including ours and laparotomy was performed in one case. In three cases without surgical treatment, free air disappeared in between 7 days and one month. This conservative treatment should be the first choice for the management in patients with pneumoperitoneum in whom perforated hollow viscus has been excluded by adequate examination. The patient presented herein only had a diverticulum of a horizontal portion of the duodenum with normal mucosa in close examinations. We hypothesized that the gas may have dissected through the bowel wall, initially at points of mucosal weakness and then tracked along the vascular sheaths to the serosal surface, rupturing into the retroperitoneal space. The gas may have then entered the peritoneal cavity through the foramen Winslow or via a rupture along the mesentery, similar to the passway that intrathoracic sources cause pneumoperitoneum.[6] In conclusion, we reported a usual case of spontaneous pneumoperitoneum, which was complicating the duodenal diverticulum, that we successfully treated non-surgically. Conservative care should be performed in similar situations, especially in an elderly patient like our patient, when there are no other associated findings to suggest peritonitis, or when there are reasonable causes of spontaneous pneumoperitoneum. We believe that this report may help to identify those patients who can safely be treated without operation, thus diminishing a negative diagnostic laparotomy. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06026t1.jpg] [is06026f2.jpg] [is06026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}