 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
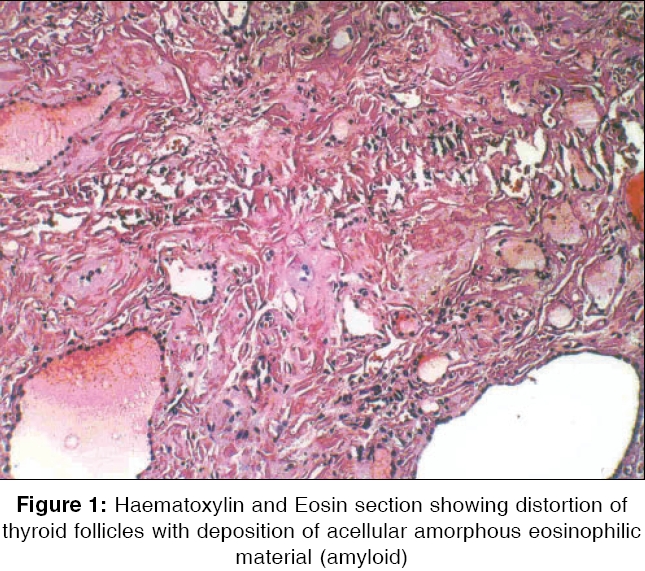
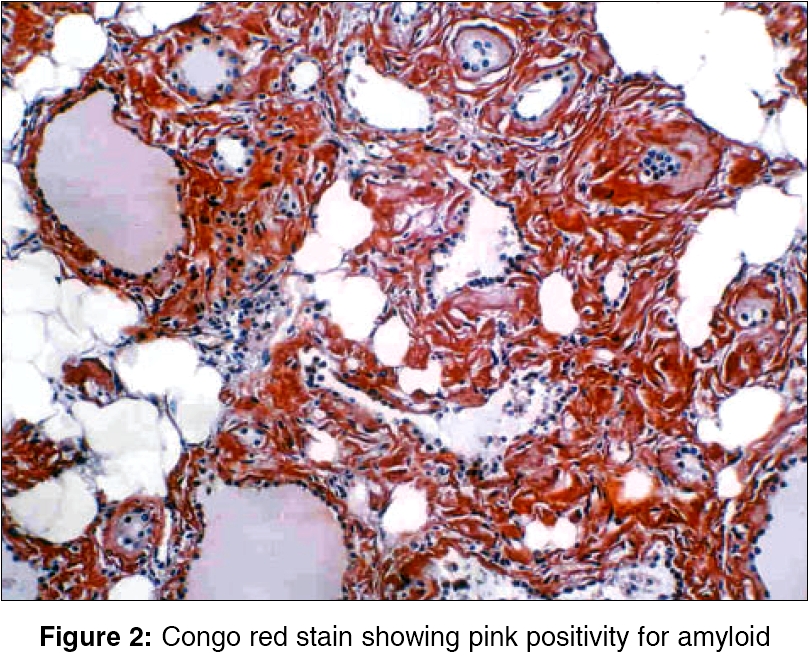
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 104-105 Case Report Amyloid goitre: A rare case report Khullar Rajesh, Sharma A, Goel A, Bagchi N, Soni V, Baijal M, Chowbey PK Department of Minimal Access Surgery, Sir Ganga Ram Hospital, New Delhi Code Number: is06028 Abstract Amyloid goitre is a rare disease which occurs in association with both primary and secondary amyloidosis. This condition has to be distinguished from other types of goitre and malignancy. Medical intervention has not been effective for amylodosis. Inspite of extensive involvement, patients are usually euthyroid and diagnosis is established on histopathological evaluation. Medical intervention has not been an effective tretament for amylodosis. Surgical intervention is necessary to relieve the symptoms of neck mass and establish a diagnosis. We report a case of a 44-year-old lady with amyloid goitre. Keywords: Amyloidosis, goiter, thyroidectomy, euthyroid. Amyloid Goitre is defined as a symptomatic mass or a clinically detectable thyroid enlargement, because of amyloid deposition. The presence of amyloid in association with thyroid gland enlargement is seen in medullary carcinoma of thyroid, in 50-80% of case.[1] Amyloid goiter occurs in association with both primary and secondary systemic amyloidosis, more commonly in the latter.[2] It is a rare entity and should be suspected in patients who are known to have diseases predisposing to amyloid deposition. The diagnosis of amyloid goitre should be suspected in patients with a diffusely enlarging thyroid gland and in those with an appropriate clinical history.[3] Peroperatively, for thyroid swellings which are soft in consistency and vascular a clinical suspicion of amyloid goitre should be made and frozen sections should be sent. We report a case study of a 44-year-old woman with amyloid goitre. Case Report A 44-year-old lady presented with a large goitre, which was gradually increasing in size for 17 years. There was no history of pain, hoarseness, or any pressure effects. The patient was euthyroid; routine haematological and biochemistry were normal. Fine needle aspiration cytology (FNAC) revealed nodular goitre. After pre-operative work-up, a bilateral subtotal thyroidectomy was performed, preserving the parathyroid glands and recurrent laryngeal nerves on both sides. Preoperatively, both lobes and isthmus were enlarged, soft in consistency and very vascular. Postoperatively, the patient had an uneventful recovery. The histopathology report stated that the normal lobular structure of the thyroid was lost and that there was decrease in the number of follicles. There was presence of a pink amorphous homogenous material between the follicles [Figure - 1], which stained positive for Congo red [Figure - 2] and methyl violet and showed green birefringence on polarization. A diagnosis of amyloidosis of thyroid was made.Discussion Amyloid infilteration of the thyroid gland in patients with systemic amyloidosis was first reported by Rokitansky in 1855, and later confirmed by Virchow and others.[2] These deposits are frequently seen at the microscopic level and have little clinical significance. Beckmann first reported the presence of clinically detectable thyroid enlargement because of amyloid deposition in 1858, followed by Eiselberg in 1904, who later coined the word ′Amyloid Goiter′.[2] Once amyloid goiter was recognised as a specific entity, around 140 cases had been reported till 1993.[4],[5] Amyloid goitre generally presents with a rapidly growing neck mass causing pressure symptoms for hoarseness. In contrast to malignant thyroid tumors that are often unilateral, amyloid goitre affects in a bilateral and diffuse manner. Patients are usually euthyroid, despite extensive involvement of the gland. FNAC may facilitate the diagnosis of amyloid goiter, but may be inconclusive in some cases.[6],[7] Surgical intervention serves to establish a diagnosis, as well as for relieving the symptoms associated with the large neck mass. Definitive diagnosis of amyloid goitre rests on the histologic evaluation of the resected specimen. In a review by Levillain etal, 56% of cases of amyloid goitre were caused by secondary amyloidosis.[7] Amyloid goitre in secondary amyloidosis is characterized by deposition of amyloid; a protein in the gland associated to atrophic follicles.[8] Uncommonly, amyloid goitre can present as a first manifestation of systemic amyloidosis.[9] No medical treatment has been effective for amyloidosis, though the overall prognosis is better with patients with secondary amyloidosis. However, in Familial Mediterranean fever, Colchicine treatment may prevent amyloid deposition.[10][11]References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06028f1.jpg] [is06028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}