 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
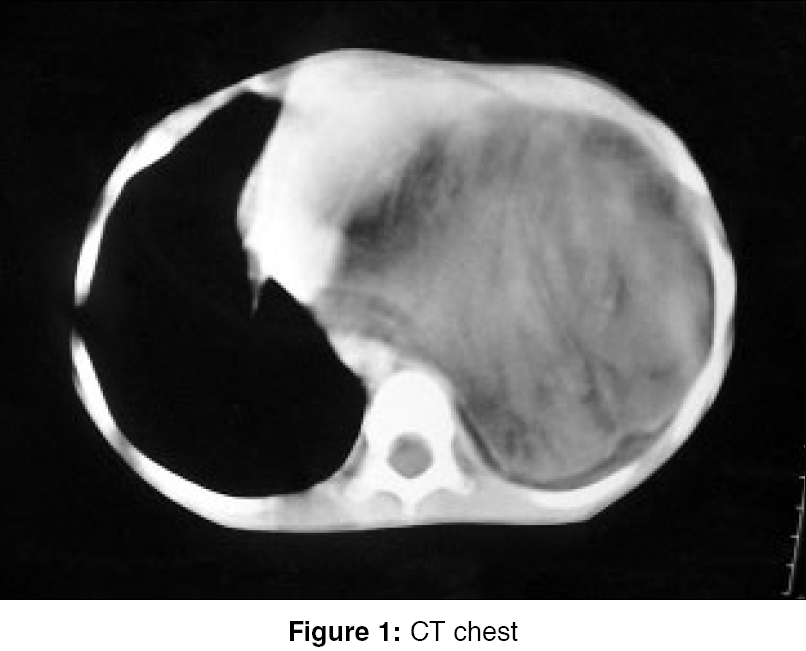
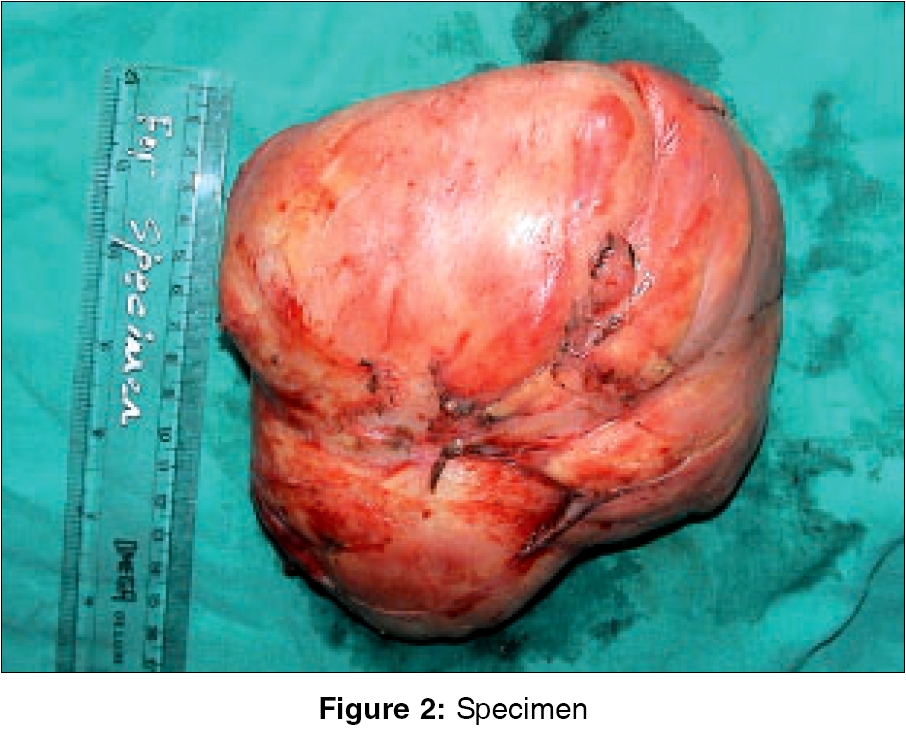
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 108-110 Case Report Giant mediastinal lipoblastoma: A case report with review of the literature Thakur Binay, Shan ZC Department of Surgical Oncology, BP Koirala Memorial Cancer Hospital, Bharatpur Code Number: is06030 Abstract Lipoblastoma is a rare benign tumor that occurs in infancy and early childhood, accounting to less than 1% of all childhood neoplasms. About 20 cases of mediastinal lipoblastoma have been reported in English literature. We report a rare case of mediastinal lipoblastoma in a 6-year-old boy. The tumor weighing 996 gm was successfully excised. Clinical manifestations, radiological and histopathological findings and treatment of this lesion are discussed.Keywords: Lipoma, lipoblastoma, lipoblastomatosis. Lipoblastoma is a rare benign tumor that occurs in infancy and early childhood, accounting to less than 1% of all childhood neoplasms.[1] This tumor commonly arises from the limbs and trunk and involvement of the mediastinum is extremely rare. Lipoblastoma is rapidly growing and complete surgical excision is recommended; there are reported recurrences after inadequate excision. In this article, we describe a rare case of mediastinal lipoblastoma in a 6-year-old boy. Case Report A 6 year old boy presented to our hospital with chief complaints of dry cough, occasional fever and shortness of breath on minimal exertion, for the last two years. There was no history of haemoptysis, chest pain, loss of weight or appetite. Personal and family history was unremarkable. His general examination was unremarkable. Examination of chest revealed minimal bulging of anterior chest wall and a dull percussion note in the left hemithorax with absent breath sounds over it. His complete blood counts and biochemical analysis of blood were within normal limits. Computed tomography (CT) of chest revealed a huge heterogeneous mass with a density of fat and mostly of soft tissue (13-24 HU), occupying almost two-third of left hemithorax. The mass was causing compression of the left lung parenchyma and shifting of mediastinal structures to right [Figure - 1]. Transthoracic (USG guided) fine-needle aspiration cytology was done four times and the report suggested an inflammatory lesion with minimal atypia each time. With a possible diagnosis of mediastinal sarcoma, the patient underwent left posterolateral thoracotomy through the sixth intercostal space, with division of the rib cage. There was a 22 x 21 x 15 cm bosselated, firm and yellowish mass adhered to left lower lobe [Figure - 2]. The mass was well encapsulated, without invasion into the surrounding structures. It was compressing ipsilateral lung, with collapse of almost two-thirds of the lung. A complete excision of the mass was achieved. The tumor weighed 996 gm. Microscopically, the tumor consisted of a lobulated mature adipose tissue, with loose fibrous septa. Some lobes contained myxoid and immature adipose tissue with immature stellate to spindled mesenchymal cells and multivacuolated lipoblasts. The histopathological diagnosis was lipoblastoma. The postoperative course was uneventful and no recurrence has been noted in follow-up of 6 months.Discussion Lipoblastoma and lipoblastomatosis are rare benign tumors arising from the fetal embryonal white fat. Chung and Enzinger[2] in 1973, suggested the term benign lipoblastoma to be used for the circumscribed type and the term lipoblastomatosis for the diffuse multicentric type of this neoplasm. These tumors generally are benign and there have been no reports of metastasis. They commonly arise from extremities (30-70%) and trunk (20-50%).[2],[3] To date, 169 cases of lipoblastoma and lipoblastomatosis have been reported in English literature. To our knowledge, about 20 cases of mediastinal lipoblastoma have been reported till date, in English literature.[1],[4],[5],[6] Though a preoperative diagnosis might sometimes prove beneficial to plan the treatment modality, it may not be fruitful, as shown in our case. Recently, Ching and colleagues showed that USG guided transthoracic biopsy is a safe procedure and it should be considered to establish the preoperative diagnosis.[7] From the imaging point of view, lipoblastoma has variable appearances. These are most likely due to the different stages of differentiation of individual lipoblastoma, which is attributable to the variable proportion of mature adipocytes within lobules and the amount of immature peripherally situated lipoblasts, fibrous septa and myxoid tissues. The two most common appearances of lipoblastoma are well-defined fatty mass and circumscribed soft tissue lesions embedded within large masses of fatty tissues.[8] Histopathologically, lipoblastoma consists of lobulated adipose tissue with fibrous septa and possesses eosinophilic mucinous to myxoid stroma with immature adipocytes, which include poorly differentiated stellate to spindled mesenchymal cells, multivacuolated lipoblasts and nearly mature adipocytes.[3] Pleomorphism and cytological atypia are lacking, but mitotic activity may be seen. Other fat tissue tumors also have histological similarities to lipoblastoma. Lipoma, fibrolipoma and angiolipoma have lobules with fibrous septa but lack of lipoblasts.[7] Hibernoma also displays a lobular pattern, but consists entirely of brown fat cells with eosinophilic, granular cytoplasm. Myxoid liposarcoma has lobulation and myxoid stroma, but it may be rare in children, mainly after 15 years old and there is a significant degree of cellular pleomorphism with nuclear atypia, atypical multivacuolated lipoblasts and atypical mitotic figures.[3] The management of mediastinal lipoblastoma is still mainly surgery. Although the lesion is considered as biologically benign, it can grow locally to an impressive proportion and lead to a significant mass effect. The tumor can cause recurrent chest infection, dyspnoea, respiratory distress, or even asphyxia, due to compression on trachea or bronchi. Death may result if expedient surgical removal is not undertaken.[5] Therefore, complete surgical excision is the treatment of choice. Local recurrences are reported in 14% to 25% of the lipoblastoma and lipoblastomatosis cases and they have been attributable to an incomplete excision.[3] References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06030f2.jpg] [is06030f1.jpg] |
| |||||||||

{kind=link}
{kind=link}