 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
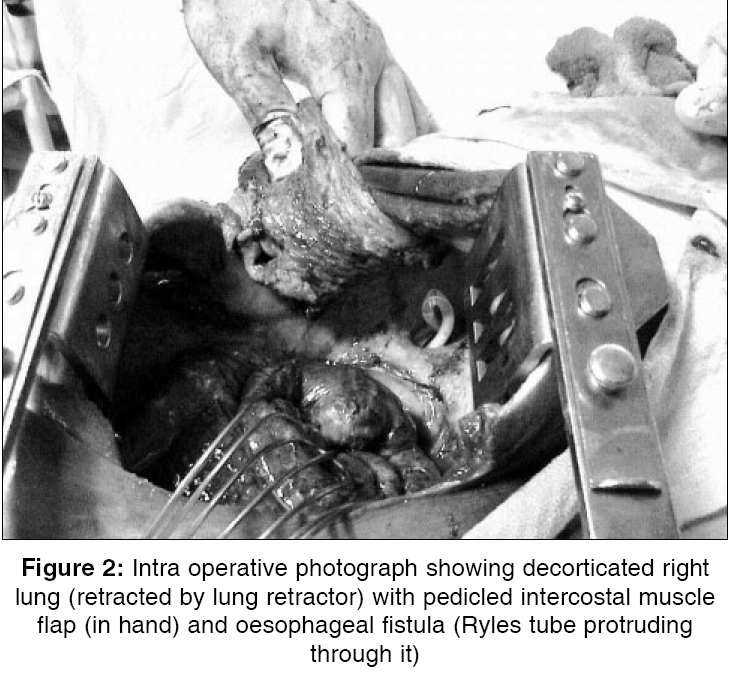
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 111-112 Images in Surgery Spontaneous oesophago-pleural fistula with empyema Darbari Anshuman, Tandon S Department of Thoracic and Cardio Vascular Surgery, K. G. M. University, Lucknow Code Number: is06031 A 20 year old debilitated male patient with a spontaneous non-tubercular oesophago-pleural fistula with right-sided empyema, is presented. After inserting a right-sided intercostal chest drain for empyema drainage, he was passing ingested liquids and food particles via this. Barium swallow study showed a fistulous tract from the upper oesophagus, to the right-sided pleural cavity [Figure - 1]. After finding this, oral intake was stopped immediately and intra venous fluid supplementation with antibiotics was started. As the results of the Barium swallow study had already confirmed the fistulous tract and due to an obviously large fistula, no other investigation was done. Pus culture via drainage tube showed growth of ′Proteus Mirabilis′. No manipulations to insert the nasogastric tube, were done. After right posterolateral thoracotomy, a thick fibrinous peel over the lung, was found. After removing the adhesions on the upper medial aspect of the right lung, a large oesophageal fistula was found with the help of nasogastric Ryle′s tube. Operative closure of the fistula by pedicled intercostal muscle flap with right lung decortication, was done [Figure - 2]. Nasogastric tube remained in situ. No other pathology was found. No lymphadenopathy or caseation was found. Pleural biopsy was nonspecific. The patient recovered after two months of conservative management and nasogastric nutritional supplementation. Because of minor leak persistence, considerable morbidity occurred. This case is unusual, because of spontaneous development of this rare type of fistula and no primary cause was found. Because of the close anatomic relationship between the esophagus and the pleura, abnormal fistulas may develop between these structures, owing to a variety of benign and malignant processes. Oesophago pleural fistula is very uncommon in clinical practice. It is a rarer condition than other oesophago-resiratory fistulas.[1],[2] Oesophago pleural fistula is commonly associated with advanced oesophageal carcinoma, oesophageal tuberculosis,[3] surgical procedures (especially postpneumonectomy),[4] endoscopic examinations and chemical injury after ingestion of corrosive substances and radiation therapy. The radiographic findings that suggest the occurrence of oesophago pleural fistula, include air in the pleural space or hydropneumothorax, or both. Barium study and CT scan confirmed it. Highlighting points
References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06031f1.jpg] [is06031f2.jpg] |
| |||||||||

{kind=link}
{kind=link}