 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
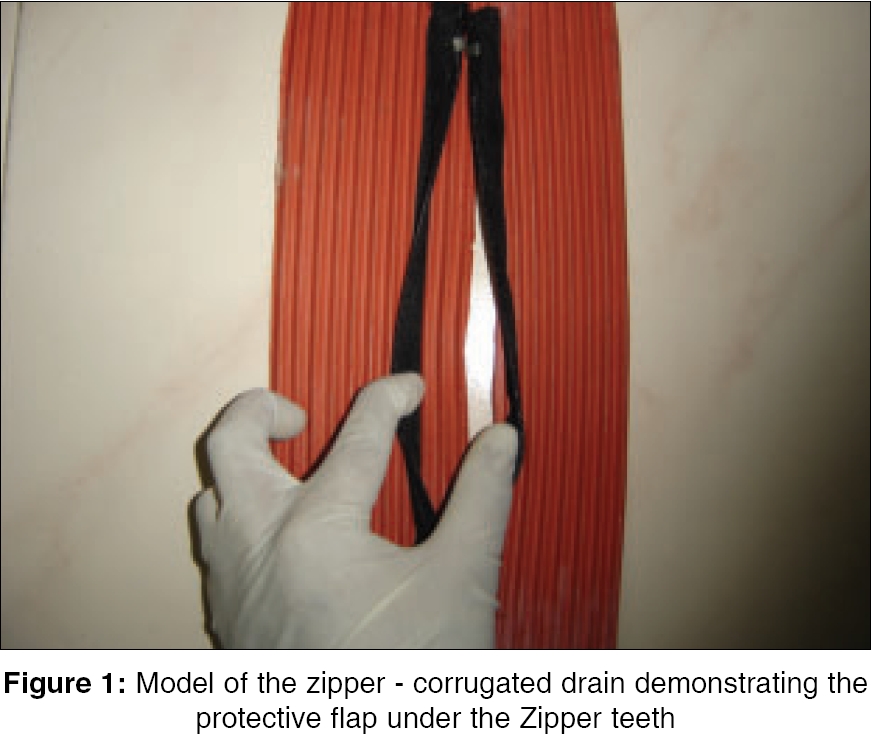
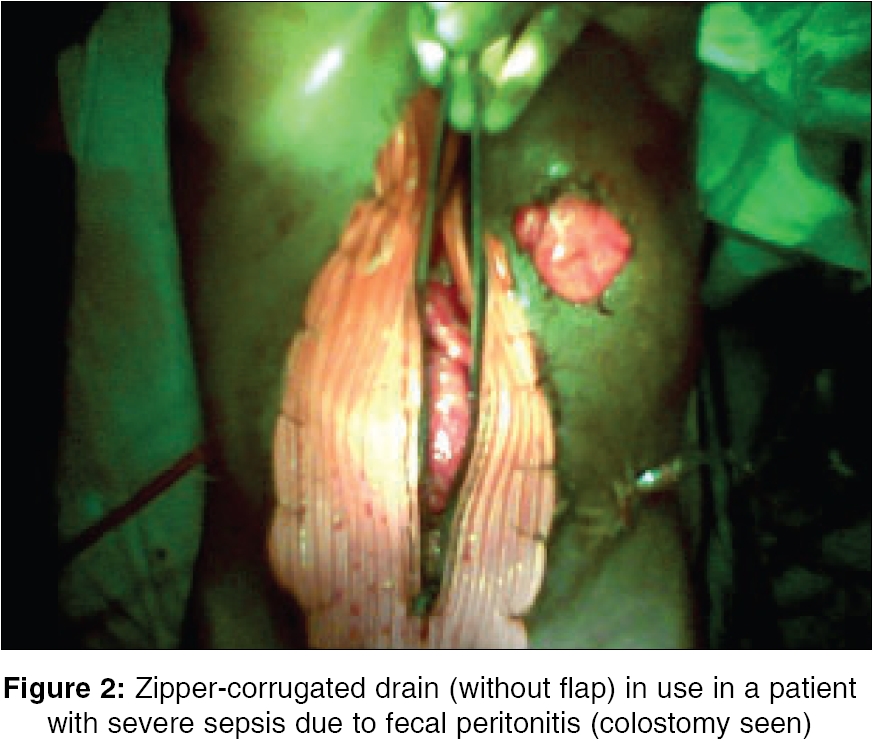
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 115-116 Point of technique Zipper-mesh laparostomy with corrugated drain at a district hospital Dasari Manoj BobbyV, Rao Harish, Ballal Rajesh Dept. of General Surgery, Govt. Wenlock District Hospital, Kasturba Medical College, Mangalore, Karnataka Code Number: is06033 Ever since laparostomy was popularized in the 1980s for necrotizing pancreatitis and severe intra-abdominal sepsis, various methods have been described by authors, though no one was proved to be better than the other. Initially, abdomen was left open and packed,[1] followed by the development of many innovative approaches - polyurethane foam, betadine packing with body binders by the French,[1] corrugated rubber drain,[2] Marlex mesh to close the abdomen without tension in patient with diffuse peritonitis,[3] the zipper modification of classical laparostomy popularized by Lequit.[4] Zipper-meshes {Polypropylene, Poly tetra fluro ethylene[5] (PTFE)} are used by many authors.[1],[6] Development of fistulas has prompted to provide a flap under the zipper teeth[5] to protect the underlying viscera. We describe another modification of the Zipper-mesh laparostomy using a corrugated rubber drain. Technique A corrugated rubber drain sheet was used with a zipper of length five centimeters less than that of the existing laparotomy incision (to match the size of laparotomy wound along with drain sheet). A vertical slit was made in the center of the sheet and Zipper was hand-sewn to the cut ends, creating a flap under the Zipper teeth [Figure - 1] and sterilized. The overall size was trimmed according to wound size and was sutured to the skin edges all around with 1'0 Nylon interrupted sutures. This provides a regular access for inspection of abdominal cavity and its lavage to avoid further sepsis [Figure - 2]. Discussion The technique of laparostomy was explored based on the fact that undrained necrotic tissue or septic foci contribute to continued activation of host processes that in turn lead to multiple organ failure and death.[6] Laparostomy as such has potential complications - massive fluid and protein loss, wound infections and hernias. However, patient selection for any kind of laparostomy is critical and appears to be more useful for those within APACHE II scores 15-30.[6] Zipper laparostomy was found to be a better technique for regular access, inspection, debridement and lavage of critically ill patients with necrotizing pancreatitis or severe intra-abdominal sepsis.[5],[6] The problems encountered with standard zipper are[5]:
Zipper-mesh technique was developed to overcome the above problems, but there were omental and bowel adhesions to the polypropylene mesh. Applying an opsite sheet under the mesh, use of PTFE mesh with a flap are the various methods described to overcome this problem. One additional problem we encountered was the cost factor involved. The commercially available zippers, polypropylene mesh with zipper, PTFE mesh are not affordable by many of our patients at the district hospital. This forced us to innovate the above described technique with a corrugated rubber drain. We did not come across any additional complications by using this technique. Moreover, we did not encounter any adhesions or trauma caused by Zipper (because of the protective flap) and the cost factor was overcome. We find this as a good alternative to the zipper-mesh. A word of caution: Select the patients carefully. In patients with severe raised intra-abdominal pressure, compression of bowel against the rubber drain sheet (even polypropylene mesh) promotes bowel ischemia and fistula formation. Acknowledgment Dr. Rupen Shah, postgraduate student, for helping us in the making of the Zipper-corrugated drain for laparostomy.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06033f2.jpg] [is06033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}