 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
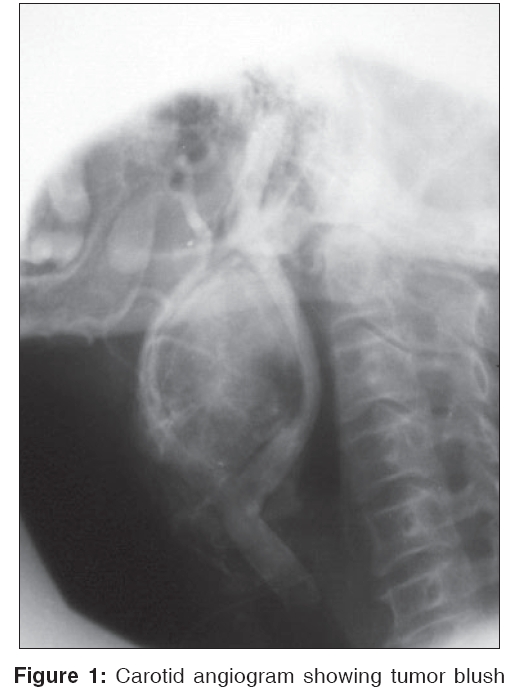
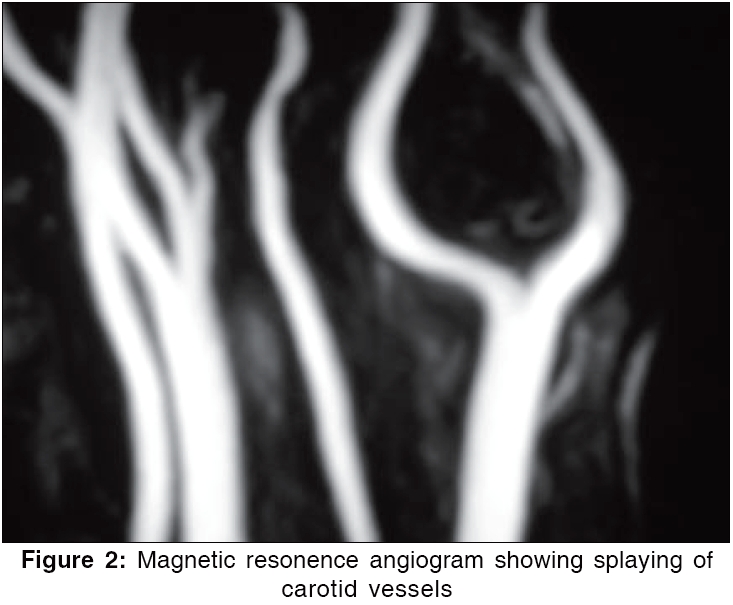
Indian Journal of Surgery, Vol. 68, No. 3, May-June, 2006, pp. 146-149 Original Article Surgical management of the carotid body tumors Mohammed Akbar Bhat, Mohammed Inam Zaroo*, Ghulam Nabi Lone Departments of CVTS and *Plastic Surgery, Sheri Kashmir Institute of Medical Sciences, Soura, Srinagar, Jammu & Kashmir, India Code Number: is06041 Abstract Background: Carotid body tumors (CBT) arise from paraganglia tissue concentrated in the neck region. Chronic hypoxia and mutations in oxygen-sensing genes are responsible for etiopathogenesis of CBT and other paragangliomas. These uncommon tumors are usually benign but may occasionally produce local and distant metastasis. Surgical excision is the only curative treatment for these cervical paragangliomas.Materials and Methods: The records of the patients undergoing surgery for CBT between January 1994 and January 2004 were analyzed. Eleven patients with a mean age of 32 years (range 21 to 48 years) were operated during this period. Patients were diagnosed by fine needle aspiration cytology, carotid angiography, color flow doppler ultrasonography and/or Magnetic Resonance angiography. Results: Complete resection of the CBT was performed in all the patients. One patient had excessive bleeding due to a tear at common carotid artery bifurcation, which was successfully salvaged. There was one death due to intracerebral hemorrhage, secondary to accelerated hypertension. There were no postsurgical neurovascular sequelae in the other 10 patients. Conclusion: Patients with CBT should be operated at an early stage of evolution. Improved imaging, vascular surgical techniques and understanding of the disease have vastly improved outcomes for these patients. CBT patients can be operated with low risk of morbidity and mortality. Keywords: Carotid artery, carotid body, glomus, paraganglioma, tumor Carotid body tumors arise from accumulations of chemoreceptor cells or glomera (nonchromaffin staining paraganglion cells) in the neck region, which develop from neural crest region during embryogenesis.[1] These uncommon neoplasms are also known as chemodectomas, paragangliomas or glomus tumors. Unresected cervical paragangliomas grow relentlessly and tend to encase the adjacent neurovascular structures, making delayed surgery more hazardous. These tumors are usually benign but can occasionally produce local and distant metastasis.[2] Evidence of local invasion and distant metastasis remain the only criteria of malignancy, as histology cannot distinguish between benign and malignant chemodectomas.[3] Chronic hypoxia has long been recognized as an etiology of CBT and other paragangliomas. Recent biogenic discoveries reveal that mutations in oxygen-sensing genes are another etiology, accounting for approximately 35% of cases and that these two etiologies are probably additive.[4] Paragangliomas of the neck are sometimes familial, bilateral and associated with other neoplasms. Complete surgical excision is the only curative treatment of these cervical tumors.[5] Materials and Methods Between January 1994 and January 2004, 11 patients were operated for carotid body tumors at Sheri-Kashmir Institute of Medical Sciences, Srinagar, Kashmir. The records of all the patients admitted for surgical intervention are maintained by the Department of Medical Records as a computerized database. The case records of the patients with CBT were retrospectively studied with approval from our institutional Review Board. There were 8 males and 3 females with a mean age of 32 years (range: 21 to 48 years). All the patients presented with slowly enlarging neck mass. Two patients had neck mass associated with local dull ache. None of the patients had bilateral disease. Evaluation of the patients included physical examination, fine needle aspiration cytology (FNAC), vascular doppler ultrasonography and/or carotid angiography [Figure - 1]. FNAC provided presumptive diagnosis in 9 patients and was equivocal in 2 patients. Only 1 patient had undergone inadvertent biopsy at a rural primary health center and the procedure had been abandoned there due to excessive bleeding from the lesion. Contrast CT scan was performed in 3 cases and magnetic resonance angiography (MRA) in 4 patients [Figure - 2]. Ten patients had normal urinary vanillyl mandelic acid (VMA) levels. One patient had preoperative hypertension along with 24 h urinary VMA excretion of 12.6 mg (normal: 1.8-9.0 mg). The patients were operated under general anesthesia. Since exposure is critical in successful removal of these tumors, a longitudinal incision was used extending from the ear lobule to the suprasternal notch along the anterior border of sternocleidomastoid muscle. After exposure of the common carotid artery, dissection was extended cephalad to the bifurcation where the caudal limits of the tumor were encountered. Carotid vessels were looped proximally and distally for manipulations during tumor dissection. The tumor was isolated from the underlying carotid vessels by dissecting along the sub-adventitial plane of the vessels. All the feeding arteries to the tumor were either coagulated or divided after ligation [Figure - 3]. Care was taken not to occlude carotids for more than 1 min to prevent iatrogenic cerebral dysfunction. Distal control of the internal carotid artery (ICA) could not be achieved in 3 patients (Shamblin type III).[6] The tumors were dissected off the ICA, being strictly in the subadventitial plane and securing the bleeders with bipolar cautery. If at any time, excessive bleeding occurred from the artery or the tumor, it was controlled with pressure on the distal aspect of the tumor along with a temporary clamp on the proximal artery. Continuous monitoring of distal ICA pressures was utilized in large tumors only where distal control of the ICA was not possible. A fine polyvinyl catheter was introduced into the ICA just beyond the bifurcation of CCA and secured with a purse-string suture. The length of the catheter within the ICA was approximately equal to the distance between the CCA bifurcation and the tympanic plate, such that the distal end of the pressure-monitoring line remained beyond the presumed distal margin of the tumor. Temporary occlusion of the proximal ICA gives the internal carotid back pressure (ICBP). If the ICBP is more than 60 mmHg, continuous monitoring of the ICA is not mandatory. Results The carotid body tumors were resected completely in all the 11 patients. The three-stage classification of Shamblin et al was used to grade the difficulty of resection.[6] Three patients were having type I tumors, 7 patients type II tumors and 3 patients type III tumors. Two patients had ICBP less than 50 mmHg on carotid occlusion test and the distal control of the ICA could not be achieved before tumor excision; their distal ICA pressures were continuously monitored during tumor dissection. Intraoperative shunting was not required in any patient. However, in 1 patient, external carotid artery was sacrificed for complete excision of the tumor. The pathological specimens ranged from 1.2 x 1.5 x 3 cm to 4.5 x 4.1 x 7 cm. Histologically, margins of the resection were free from disease in 9 patients and indeterminate in 2 cases. One patient developed accelerated hypertension leading to intracerebral hemorrhage during surgery and died 36 h after surgical intervention. The patient had a secreting paraganglioma of neck and his 24 h urinary VMA excretion was 12.6 mg (normal 24 h urinary VMA excretion: 1.8-9.0 mg). There was temporary hypoglossal nerve paresis in 1 patient, which recovered within 3 days. One patient had temporary hoarseness of voice (recurrent laryngeal nerve paresis), which recovered within a period of 6 weeks. The average blood loss during the operation was 200 ml (range: 100 to 550 ml). Only 1 patient had excessive blood loss (>500 ml) due to a tear at common carotid artery bifurcation, which was repaired after temporary occlusion of the carotid vessels. The patient did not have any postoperative adverse sequelae.Discussion The carotid body tumors are uncommon, accounting for only 0.03% of all neoplasms and 0.06% of head and neck tumors. The only curative treatment for paragangliomas of the neck is complete surgical excision.[5] The morbidity associated with unresected tumors is significant and includes progressive lower cranial nerve palsies, dysphagia, airway obstruction, extension to the skull base with infiltration of the central nervous system and possible malignant change. The best way to minimize the rate of complications is to operate them at an early stage of evolution.[7] Precise determination of tumor sites and its relations with adjacent structures is essential since it influences the therapeutic strategy.[8] Any patient presenting with an enlarging mass near in upper posterior triangle of neck should be evaluated to rule out CBT. Preoperative biopsy is hazardous and should not be attempted. Current modalities for evaluating the paragangliomas of the neck include color flow ultrasonography, computed tomography (CT), carotid arteriography, digital subtraction angiography (DSA), magnetic resonance angiography (MRA) and FNAC.[3],[9] High-resolution contrast-enhanced CT best shows the extent of the disease and involvement of the surrounding structures. MRA demonstrates tumor vascularity and three-dimensional relationships of the tumor to surrounding vascular structures [Figure - 2]. Angiography reveals the vascular extent of the tumor, the carotid artery involvement, size and location of the tumor-feeding vessels and the possibility of performing a preoperative embolization.[3],[10] Arteriography also allows evaluation of coexistent atherosclerotic disease of the carotid arteries [Figure - 1]. Sykes and Ossoff[11] effectively summarized the standard principles in the surgical management of these tumors: 1) Wide surgical exposure, 2) proximal and distal vascular control, 3) identification and preservation of neurovascular structures, 4) subadventitial tumor dissection, 5) dissection of tumor from internal and external carotid arteries, 6) ligation of the external carotid artery when necessary and 7) vascular shunting and grafting wherever necessary. Better surgical exposure of the nerves and vessels complemented with intraoperative neurophysiological monitoring are vital to maintain anatomical and physiological function of the involved nervous and vascular structures. The reported rate of perioperative cerebrovascular accidents is less than 1% in recent reports.[10] The incidence of cranial nerve deficits ranges from 22 to 49% and such deficits continue to be the most important cause of postoperative morbidity.[7],[10],[12] Cranial nerve deficits can manifest at the time of presentation or occur after tumor resection. In the present series, two (18.18%) patients had temporary cranial nerve injury {paresis}. Both of them had Shamlin type III tumors. In our opinion, this complication can be reduced by better understanding of the anatomic course of the nerves and an aggressive effort to preserve them during tumor resection. Intraoperative sacrifice of cranial nerves becomes necessary in some cases. In our series, none of the patients required sacrifice of a cranial nerve. It is important to appreciate the risk of massive blood loss. Major feeding arteries are usually encountered within 2 cm of the carotid bifurcation and most of the vascular injuries are encountered in this area. Blood salvage for autotransfusion in the presence of tumor is not usually done, but controlled deep-inhalation anesthesia and sodium nitropruside induced hypotension may be useful to decrease the blood loss.[13] Preoperative embolization should be used in large tumors to reduce the vascularity, thereby decreasing the blood loss and morbidity. Embolization runs the risk of stroke and should be performed only by highly qualified personnel.[14],[15] Shamblin classified the cervical paragangliomas into three groups, as per the difficulty of surgical resection. Group I tumors are localized and easily resected (not involving surrounding vessels), group II include tumors adherent or partially surrounding vessels and group III paragangliomas intimately surround or encase the vessels.[6] In our series, only 1 patient had type I, 7 patients (63.6%) type II and 3 patients (27.27%) type III paragangliomas. The endocrine capability of the tumor (1-4%) should be kept in mind while dealing with hypertensive patients.[3] There might be elevation of blood pressure during surgical manipulation of the tumor. In our series, there was one death due to accelerated hypertension with intracerebral hemorrhage secondary to secreting CBT. The patient had accelerated hypertension despite being on alpha blockade (phentolamine) and beta blockade (atenolol) perioperatively. Continuous invasive arterial pressure monitoring with more rigid control of blood pressure perioperatively may be helpful in preventing this catastrophe. All the patients do suffer from short periods of cerebral hypo-perfusion while manipulating the carotid arteries. Therefore, monitoring the adequacy of cerebral perfusion using electroencephalogram, somatosensory evoked responses, arterial stump pressure assessments, transcranial doppler measurement of middle cerebral artery flow velocities or possibly direct measurement of cerebral blood flow is recommended.[16],[17] When carotid artery cross-clamping is required, one should monitor cerebral function and be prepared to use an indwelling carotid shunt to maintain cerebral perfusion. However, none of the patients in this series required a carotid shunt for tumor excision.[17] Continuous monitoring of ICA pressures was performed only in two patients who had ICBP less than 50 mmHg and where distal control of ICA was not possible.This technique allows the surgeon to take corrective measures as soon as the ICA pressures fall below a critical level. Although the internal carotid artery can be safely sacrificed if the distal arterial stump pressure is more than 65 mmHg, the surgeon should always aim at restoration of the carotid artery integrity either by repair or reconstruction.[17] References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06041f3.jpg] [is06041f1.jpg] [is06041f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
![[Figure - 3]](/showimage?is/photo/is06041f3.jpg){kind=link}