 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
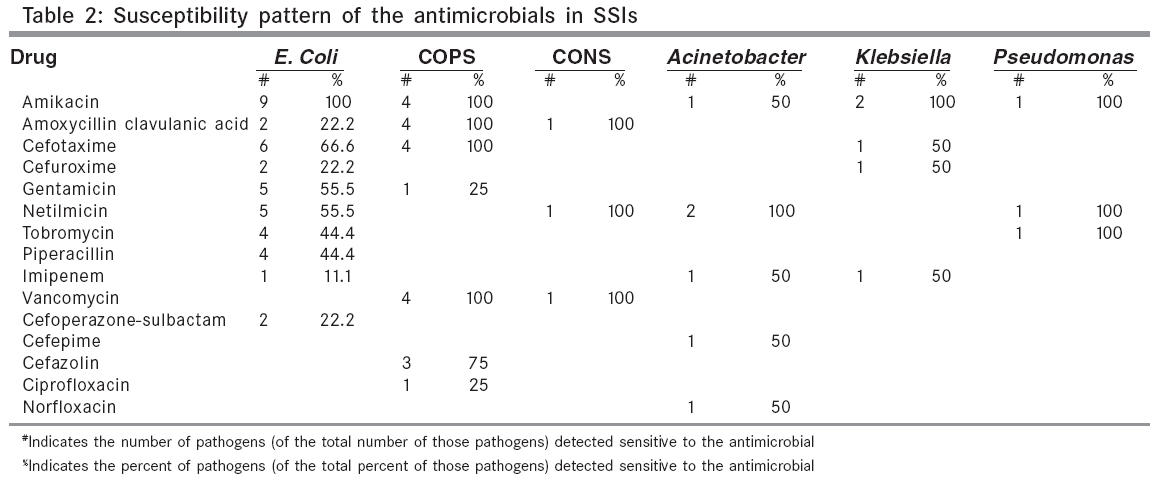
Indian Journal of Surgery, Vol. 68, No. 3, May-June, 2006, pp. 150-156 Original Article Survey and evaluation of antibiotic prophylaxis usage in surgery wards of tertiary level institution before and after the implementation of clinical guidelines Sohil Ahmed Khan, Padma G. M. Rao, Anand Rao*, Gabriel Rodrigues* Department of Pharmacy Practice, Manipal College of Pharmaceutical Sciences and *Department of Surgery, Kasturba Medical College, Manipal - 576104,, Karnataka, India. Code Number: is06042 Abstract Background: Wound infections are the commonest hospital-acquired infections in surgical patients. Approximately 30-50% of antibiotic use in hospitals, is now for surgical prophylaxis. However, between 30-90% of this prophylaxis is inappropriate, that increases the selective pressure favoring the emergence of antimicrobial resistance. Judicious use of antibiotics in the hospital through effective antibiotic policy and guideline development is thus essential.Aims: To prepare a guideline for surgical antibiotic prophylaxis and to evaluate the impact of it in clinical practice. Settings and Design: A retrospective and prospective study was carried out over a nine month period, in a surgical unit of a tertiary care institution. Materials and Methods: An antibiogram was prepared to evaluate the sensitivity pattern retrospectively. A prospective study was done to evaluate the prescription pattern of antibiotic prophylaxis and incidence of surgical site infection. A draft guideline was prepared with expertise by the surgeon. Standardized recommendations in the guideline were done by the nominal group technique. Post-recommendation evaluation was done to observe the impact of the guideline in clinical practice. Results and Conclusions: 222 cases were evaluated during the pre-recommendation period, of which 21 were infected with surgical site infections that were rated as 9.45%. Use of prophylactic antibiotics was widespread and inconsistent with published guidelines. 56 cases were evaluated during the post-recommendation period. None of the cases were infected. Prophylactic antibiotic use was consistent with respect to choice and duration. The study showed the importance of a multidisciplinary approach in implementing local guidelines in healthcare institutions, as per their hospital antimicrobial sensitivity pattern and expert's opinions. Keywords: Antibiotic prophylaxis, guideline adherence or practice guidelines, guideline, humans, nominal group technique, prophylactic antibiotics, surgical site infections, surgical wound infection/prevention and control Surgical site infections (SSIs) are the second most common cause of nosocomial infections.[1] Though the post- Listerian era is enriched with much advances in field of asepsis and surgical and antiseptic techniques, SSIs are still a threat to the surgical world. Antibiotic prophylaxis is one component of preventive strategy against SSIs, that is based on a good surgical technique, strict asepsis in the operating theatre and control of infection within the hospital or general practice.[2],[3] Although properly administered antibiotics can reduce postoperative SSIs secondary to preoperative bacterial contamination, widespread use of prophylactic antibiotics have the disadvantages of emergence of multi-resistant organisms.[4] The rich tropical climate of India additionally challenges the clinicians to manage a wide variety of infectious diseases. The higher rates of surgical site infections are associated not only with a higher morbidity and mortality, but also with increased medical costs. Hence, a constant awareness of the ever-present threat of infection must be a way of life for the entire surgical fraternity. The aims of this study were to identify the common pathogens causing infections and their sensitivity pattern, to determine the incidence of surgical site infection, to prepare guidelines for the use of surgical antibiotic prophylaxis and to evaluate the impact of the same in clinical practice. Materials and Methods The study was conducted in the department of surgery, of a multidisciplinary teaching hospital of South India, after being approved by the ethical committee. Initially a retrospective analysis of microbiological data (from medical records) of operated cases was analyzed from September 2003 to August 2004, to evaluate the susceptibility pattern of antibiotics. Subsequent follow- up chart reviews were also done to detect the incidence of SSIs. Each follow-up records were evaluated to determine the surgical site infections, that included pharmacy, microbiology, biochemistry and other lab records . Then a prospective study was carried out over an eight month period, from September 2004 to April 2005. Inpatients undergoing surgical procedures under clean and clean-contaminated category were included and those having immunocompromised conditions, patients with active infection requiring treatment before or at the time of surgery and surgical procedures under contaminated and dirty category, were excluded. An antibiogram was prepared from the microbiology ledger to identify the common pathogens involved in the surgical infections, along with sensitivity pattern. A retrospective analysis of one-year data from September 2003 till September 2004 was done. The prospective study involved data collection from patient case records and microbiology reports for demographic details and clinical details, including prophylactic antibiotic dose, duration, frequency and route. For detection of surgical site infections, the wound was inspected for any evidence of infection starting from 48 hours after surgery, to the day when the patient was discharged. Patients who underwent laparoscopic procedures were discharged on the 3rd and 4th postoperative day. The rest of the patients were discharged after the suture removal, with clinically no evidence of SSIs. The patients were called for follow-up after 1-2 weeks in case of laparoscopic cholecystectomy for the suture removal and after 15 days to a month in open cholecystectomy cases. Patients were observed during their follow-up visits in such cases. Self-reporting of infections by the patients was also encouraged, once they were discharged. The criterion for SSI was based on centre for disease control′s (CDC′s) definition of SSI. The patient who satisfied the superficial incisional surgical site infection criteria was studied. Cases were followed to know the exact time of administration of the prophylactic antibiotic in the operation theatre. The prescription pattern was evaluated with respect to choice, duration, route and frequency. Duration of hospital stay was evaluated in the infected group and non-infected group. Data collected from the study, along with evidence-based literature and microbiology reports, were clubbed together to make a draft guideline, with expertise from a surgeon. This draft guideline was circulated among the surgical staff for their feedback on the recommendations made regarding the choice and duration of antibiotic prophylaxis in surgical procedures belonging to the clean and clean- contaminated surgery. Standardization of the draft guideline was done by a nominal group technique, where each recommendation was stated, followed by the feedback results and then a discussion was initiated among the surgeons to accomplish the standardization procedure. After standardization of the guideline, a 7-15 days interval was given and then the cases were studied to evaluate the change (if any) in utilization of surgical antibiotic prophylaxis. Results (A) Antibiogram study (retrospective analysis) 168 cases were evaluated to prepare an antibiogram retrospectively. Escherichia coli was the most common pathogen found [42 (25%)], followed by Pseudomonas aeruginosa [35 (20.83%)] and coagulase-positive staphylococci [32 (19.04%)] in surgical set-up. Of the antimicrobials commonly used, impressive results of susceptibility pattern were observed with an aminoglycoside, amikacin (61.30%), followed by a third generation cephalosporin, cefotaxime (40.47%) and amoxicillin-clavulanic acid (33.92%). The prospective study evaluated a total of 308 cases, of which 222 belong to the pre- recommendation and 56 cases belong to the post-recommendation phase of guideline implementation. (B) Pre-recommendation phase Out of 222 patients, 102 belonged to the clean class and 120 belonged to the clean- contaminated class. 21 cases got infected, giving a surgical site infection of 9.45%. Pathogens involved in infected cases and antibiotic susceptibility pattern are mentioned in [Table - 1] [Table - 2], respectively. The cases were also evaluated for studying the prescription pattern of prophylactic antibiotic in different types of surgery. It included appendectomy [37 (16.66%)], head and neck surgery [31 (13.96%)], cholecystectomy [20 (9.0%)], laparoscopic cholecystectomy [27 (12.16%)], Exploratory laparatomy [22 (9.90%)], Trendelenburg ligation [11 (4.95%)] and hernia surgery, which includes inguinal hernia repair [22 (9.90%)], paraumbilical hernia [11 (4.95%)], incisional hernia [14 (6.30%)], hernioplasty [16 (7.20%)] and herniorrhaphy [11 (4.95%)]. The final guideline for prophylactic antibiotic use is given in [Table - 3]. 25(11.26%) cases received a single preoperative dose, in 16 (7.20%) cases, the antibiotic was stopped within 24 hours of surgery and in 181 (81.53%) cases, the antibiotic was continued for 5-7 days after surgery. In all cases, prophylactic antibiotic was administered through the intravenous route only. Prophylactic antibiotics were administered at the time of induction in the operation theatre, in all the cases. Average duration of hospital stay was found to be 16.34 days in the infected group (21 cases) and 7.43 days in the non-infected group (201 cases). (C) Post-recommendation phase A total of 56 cases were studied, of which 32 (57.14%) cases were of clean class and 24 (42.85%) were from clean-contaminated class. There was no incidence of surgical site infection. In clean surgeries like hernia, single dose amoxicillin clavulanic acid was the preferred option [12 (70.58%)]. Out of 6 Trendelenburg ligation surgeries, single dose amoxicillin-clavulanic acid [3 (50%)] and cefotaxime [3 (50%)] were the preferred options in conditions where ulcer was not present. Out of 9 cases of head and neck surgery, amoxicillin-clavulanic acid [6 (66.66%)] was the preferred option, followed by cefotaxime 3 (33.33%). Out of 24 clean contaminated surgeries , cefotaxime with metronidazole was the preferred option in 19 (79.16%) cases. Out of 56 cases, single preoperative dose were received by 22 (39.28%) cases, antibiotic was stopped within 24 hours of surgery in 32 (57.14%) cases and it was continued postoperatively for 5-7 days in 2 (3.57%) cases. All the 56 cases received prophylactic antibiotic through intravenous route. In all the 56 cases, antibiotic was administered at the time of induction in the operation theatre. Discussion Surgical site infection rate was comparable to results from other studies conducted in South and Southeast Asia. Nguyen et al[5] described an overall incidence rate of 10.9% in Hanoi, Vietnam. Sohn et al[6] documented a postoperative infection rate of 14.3% in Ho Chi Minh City, Vietnam. SSI developed in 7.6% cases, in a community-based hospital in Japan.[7] However, it is significantly higher when compared to western studies. Study of the efficacy of nosocomial infection control (SENIC) [8] shows the overall rate of SSI to be 4.1%, while Olson et al[9] documented a rate of 2.5% at the end of their study, after 10 years. The overall SSI rate was 12% in a Bolivian study[10] and around 2.6% in a Columbian study.[11] A study conducted in underdeveloped countries like Tanzania, shows the overall incidence of SSIs to be around 19.4%.[12] Surgical site infections of 16.9% were documented in Beograd, Serbia.[13] The major factors contributing to high incidence of SSIs in the present study, includes lack of barriers at the nursing outlet level and operation theatre inlet level, causing cross-contamination among the patients, leading to increased rate of infection. The standard surveillance for surgical site infections requires a 30-day patient follow-up. In the present study, only the patient who underwent laparoscopic procedures were discharged on the 3rd and 4th postoperative day. The rests of the patients were discharged after suture removal, with clinically no evidence of SSIs. The patients were called for follow- up after 1-2 weeks in case of laparoscopic cholecystectomy for suture removal and after 15 days to a month in open cholecystectomy cases. Patients were observed during their follow-up visits in such cases. Although the study cannot give the exact incidence of SSIs, the patients were properly instructed regarding chances of infections that can develop once they are discharged. Self-reporting of infections by the patients was also encouraged. In our study, a majority of the procedures belonged to biliary tract surgery, where predominance of gram-negative bacilli has been observed. High incidence of isolation of E. coli in the bile is well known. Only those cases where there was leakage of bile in the peritoneal cavity, developed SSI from biliary tract surgery in our study. Recent studies show the higher incidence of gram-negative bacilli as the cause of SSIs.[7],[11],[14] Most of the North American studies show the predominance of gram-positive cocci as the etiology of SSIs. Two Indian studies also highlight the predominance of gram-positive cocci as the etiology of SSIs.[15],[16] MRSA is an ever-increasing problem in the hospital environment, that is holding its strong presence in the community also.[17] MRSA was identified in some cases that had postoperative SSI, but later it was proved to be a skin contaminant. However, all those procedures that were excluded in our study, belonged to the contaminated and dirty class. There is need for studies highlighting the exact incidence of MRSA in the Indian set-up, along with methods to curtail it, the judicious use of antibiotics and strict aseptic measures being the major ones for the same. Cefotaxime was the most commonly used antibiotic for prophylaxis, followed by amoxicillin-clavulanic in the present study. As per the choice of prophylactic antibiotic, the American society of health system pharmacist recommends cephalosporins (first, second or third generation) based on the local sensitivity pattern, the efficacy, tolerability and costs.[18] Cefotaxime showed an impressive susceptibility pattern in the present study. However, there was a widespread use of prophylactic antibiotics. These were frequently given in multiple doses extending beyond 24 hours. Aminoglycosides were also administered as prophylaxis, that is not recommended. Prophylactic antibiotics were administered in all the cases of clean head and neck surgery, hernia surgery and elective laparoscopic cholecystectomy, that are not recommended. Antibiotic prophylaxis is indicated in such cases, when there is an involvement of insertion of prosthetic devices, that are associated with low infection risk and high morbidity. Extension of antibiotic prophylaxis to other categories of clean wounds should be limited to patients with two or more risk factors established by criteria in the SENIC, because the baseline infection rate in these patients is high enough to justify their use.[19] None of the guidelines support prolonged used of prophylactic antibiotics. Prolonged use of antimicrobial prophylaxis was common in our study, because a majority of the literature suggesting short duration of antimicrobial prophylaxis, are from developed countries. In a developing country like India, with extremely limited health care resources along with poor economic status of the patient, healthcare professionals including surgeons do not want to take any chances for infection. However, it may not be a rational reason for prolonged antibiotic use. The majority of the surgeons are still reluctant to leave this conventional practice. There is a need for change from this conventional practice of prolonged prophylactic antibiotic usage by surgeons, which they believe will help them in not taking any chance for future infection, that includes adequate measures like development of local guidelines, SSIs surveillance, educational interventions, good surgical technique and strict asepsis in the operating theatre to prevent the emergence of multiresistance organisms along with MRSA. During the post- recommendation period, the choice of prophylactic antibiotics in different types of clean and clean- contaminated surgeries was consistent with the guidelines. Patients belonging to the pre and post- recommendation phase were of a similar group with respect to demographics, risk and type or procedures. Absence of SSIs during the post-recommendation period is not solely due to appropriate antibiotic prophylaxis usage. It is a well known fact that antibiotic prophylaxis is an adjunct to and not a substitute for good aseptic procedures in the surgical environment. Most of the SSIs arise from the patient′s endogenous flora, which contaminates the wound by direct contact.[20] Preparation of the patient for surgery was done meticulously, to decrease the microbiological burden on the patient′s bowels, skin, respiratory tract or genital tract, depending on the procedure being performed. Shaving was done on the previous day of surgery. Patients were instructed to take bath and wear clean clothes on the day of surgery, as exogenous contamination of wounds is also important in the pathophysiology of SSI, particularly for clean surgical procedures, because surgeons do not incise mucous membranes or hollow viscera. Airborne bacteria originating from the patient or clothing or skin of the surgical team suffice to create SSI in these types of procedures, particularly when implants are being placed. Unless the blood sugar levels are well-controlled by Insulin administration, patients were not taken up for the surgical procedure. All horizontal surfaces were cleaned every morning before any intervention; horizontal surfaces and all surgical items (e.g., tables, buckets) were cleaned between procedures. At the end of the working day, a complete cleaning of the operating theatre was performed. Once a week, a complete cleaning of the operating room area, including all annexes such as dressing rooms, technical rooms and cupboards were done. All members of the surgical team who would work on the operating field, were educated to scrub arms and hands with chlorhexidine, iodophors or hexachlorophene for at least 5 minutes before the first procedure of the day and for 2-5 minutes between subsequent procedures. Sterile gloves of good quality were used. Gloves were changed immediately after any accidental puncture. Postoperative dressing was done only in the dressing area. Members of the surgical team entering the operating room when the operation is about to begin or already underway, wear a mask and headgear that fully covers hair, sideburns and neckline. Scrub suits covered most bare skin to decrease shedding of microorganisms from uncovered skin. As individuals shed up to 10 9 epithelial cells per day, many of which carry bacteria, all personnel working in the operating room followed this practice. Any member of the surgical team who suffered from a skin lesion such as a boil, was refrained from working in the operating room. As a part of ISO (International Organization for Standardization) standardization for the hospital, healthcare professionals were adequately trained in maintaining good aseptic techniques. The duration of prophylactic antibiotic administration changed remarkably after the standardized recommendations. During the post- recommendation phase, prophylactic antibiotics were stopped after 24-48 hours of surgery. The development of guidelines helped in effective utilization, by preventing the overuse of prophylactic antibiotics. A multifaceted educational intervention involving a team effort of healthcare professionals can have a significant effect on effective antibiotic utilization and reducing the incidence of surgical site infections. Local guidelines seem more likely to be accepted and followed than those developed nationally. Development of similar antibiotic guidelines is essential to prevent emergence of resistant pathogens, to rationalize the use of antibiotics in the most cost-effective manner and for preventing the occurrence of hospital- acquired infections. The present study has identified that the interventions done at a specific time by the teamwork of healthcare professionals, influence the prescribing appropriateness of surgical antibiotic prophylaxis. Several studies have highlighted the importance of a multidisciplinary approach in effective utilization of antibiotic prophylaxis.[21],[22] This study supports the team effort by surgeons, anesthetists, microbiologists, nurses and clinical pharmacists in the effective utilization of prophylactic antibiotics in hospital. The study also highlights the incidence of surgical site infections and prophylactic antibiotic usage in an Indian set-up. Conclusion A multifaceted educational intervention involving a team effort of healthcare professionals can have a significant effect on effective antibiotic utilization and in reducing the incidence of surgical site infections. Local guidelines seem more likely to be accepted and followed than those developed nationally. The following are the basic principles to be followed for prophylactic antibiotic usage: 1. The final decision regarding the benefits and risks of prophylaxis for an individual patient will depend on:
2. Treatment policies should be based on local information about the epidemiology of drug-resistant bacteria. Implementation of a prophylaxis policy should not trigger an automatic change in treatment policy. 3. Inappropriate prolongation of surgical prophylaxis can be reduced by use of specific order forms for surgical prophylaxis or recording of prophylaxis in single dose sections of existing drug prescription charts. 4. Patients with a history of anaphylaxis or urticaria or rash, occurring immediately after penicillin therapy are at increased risk of immediate hypersensitivity to penicillins and should not receive prophylaxis with a beta-lactam antibiotic. 5. Policies for surgical prophylaxis that recommend beta-lactam antibiotics as first line agents, should also recommend an alternative for patients with allergy to penicillins or cephalosporins. 6. Prophylaxis should be started preoperatively in most circumstances, ideally within 30 minutes of the induction of anesthesia. 7. An additional dose of prophylactic agent is not indicated in adults, unless there is blood loss of up to 1500 ml during surgery or hemodilution of up to 15 ml/kg. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06042t1.jpg] [is06042t2.jpg] [is06042t3.jpg] |
| |||||||||

![[Table - 1]](/showimage?is/photo/is06042t1.jpg){kind=link}
{kind=link}
![[Table - 3]](/showimage?is/photo/is06042t3.jpg){kind=link}