 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 68, No. 4, July-August, 2006, pp. 201-204 Original Article Histological changes in gallbladder due to stone disease Rahul Khanna, Rashmi Chansuria*, Mohan Kumar*, H. S. Shukla** Departments of Surgery, *Pathology and **Surgical Oncology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India Correspondence Address:Rahul Khanna, A-15 Brij Enclave, Sunderpur, Varanasi - 221 005, India. E-mail: dr_rahul_khanna@rediffmail.com Code Number: is06058 Abstract Gallbladder stones are known to produce histopathological changes in the gallbladder. It is also one of the predisposing factors for the development of cancer of the gallbladder.Aim: This work was carried out to study the diverse histopathological changes in the gallbladder mucosa as a result of cholelithiasis in the population of eastern Uttar Pradesh. Materials and Methods: The study was conducted on 140 consecutive gallbladders, electively resected for cholelithiasis. Of these, 80 patients had symptoms related to stone disease while in 60 patients, the gallstones were asymptomatic and incidentally detected. The specimens were fixed in 10% formalin and submitted to detailed gross examination. For microscopy after hematoxylin and eosin staining, sections were obtained from the fundus, body and neck of the gallbladder. Additional sections were taken from grossly abnormal looking areas. Results: On gross examination, it was found that outer gallbladder surface was congested in 40 patients (28.5%), wall thickness was increased in 60 (42.5%) and mucosal abnormalities were present in 90 patients (64.5%). At microscopy, epithelial hyperplasia was observed in 83 (69%), antral metaplasia in 23 (16.5%), intestinal metaplasia in 22 (15.5%), dysplasia in 12 (8.5%) and carcinoma in situ in 1 specimen (0.7%). Conclusion: Gallstones are an important risk factor for cancer of gallbladder to develop. We found that cholelithiasis and even silent gallstones which were asymptomatic produced a series of epithelial pathological changes in the gallbladder mucosa, which could be precursor lesion of gallbladder carcinoma. Keywords: Cholelithiasis, dysplasia, hyperplasia, metaplasia Introduction Cholelithiasis produces diverse histopathological changes in gallbladder mucosa - namely, acute inflammation, chronic inflammation, granulomatous inflammation, hyperplasia, cholesterosis, dysphasia and carcinoma. In endemic regions of India such as eastern Uttar Pradesh, where carcinoma of the gallbladder constitutes 4.44% of all malignancies,[1] such changes may help in understanding the pathogenesis of the malignant process. We undertook this study to evaluate the incidence of these changes in the gallbladder of patients undergoing cholecystectomy for stone disease.Materials and Methods The present work was a prospective study and was carried out on 140 consecutive gallbladders, electively resected for cholelithiasis, during an 18-month period from January 2001 to July 2002. Of these, 80 patients had symptoms related to gallstone disease while in remaining 60 patients, the stones were asymptomatic and incidentally detected on ultrasound. These asymptomatic patients underwent cholecystectomy as it is our practice to perform cholecystectomy on all patients with gallstones who are otherwise fit and have no contraindication to surgery. During the same period, 20 cases of invasive gallbladder carcinoma were also treated. Stones were found in 18 of these 20 patients with gallbladder cancer. The reseated specimens were fixed in 10% formalin and submitted to the Department of Pathology. The following parameters were noted on gross examination of gallbladder: dimensions, outer surface, wall thickness, mucosa, number and types of stones. Three sections including entire wall were obtained from the fundus, body and neck of the gallbladder. Additional sections were taken from abnormal-appearing areas. Routine processing of tissue sections with hematoxylin and eosin staining was done. On microscopic examination, following findings were recorded: hyperplasia, antral metaplasia, intestinal metaplasia, dysplasia and carcinoma in situ. The following microscopic diagnostic criteria were used:
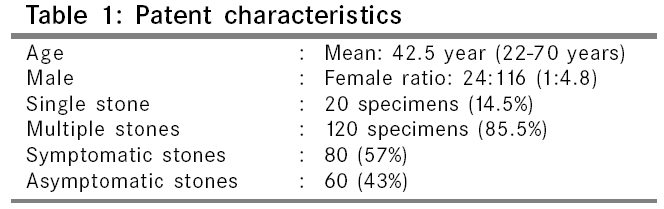
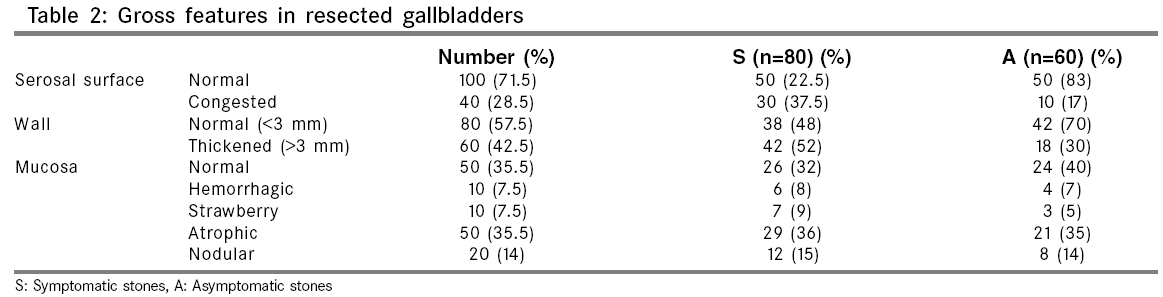
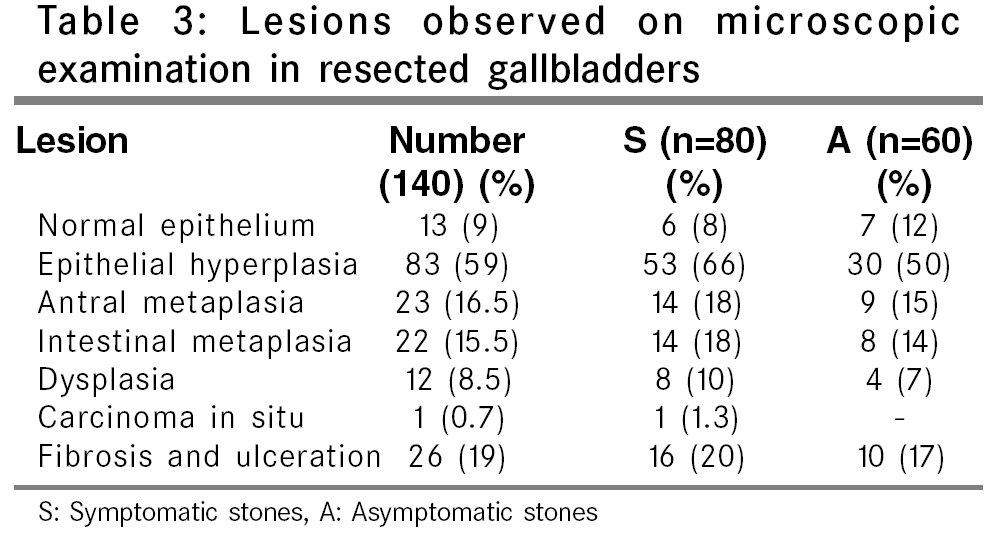
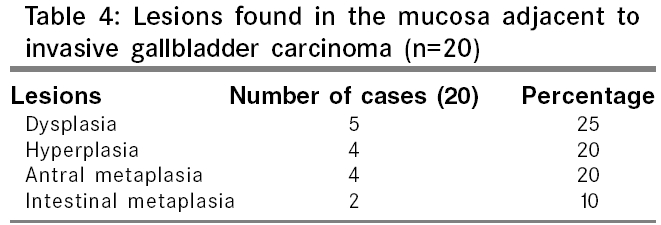
Observations Out of 140 gallbladder specimens, 116 were from female and 24 from male patients (M: F ratio 1: 4.8). The mean age of patients was 42.5 years (range 22-70). Single stone was found in 20 gallbladders (14.5%) and multiple stones in 120 (85.5%) [Table - 1]. Gross features The serosal surface of the gallbladder was found normal in 100 (71.5%) and congested in 40 patents (28.5%). Gallbladder wall thickness was normal (< 3 mm) in 80 (57.5%) and thickened (>3 mm) in 60 patients (42.5%). Mucosa was normal in 50 (35.5%), hemorrhagic in 10 (7.5%), strawberry-like in 10 (7.5%), atrophic in 50 (35.5%) and slightly nodular in 20 specimens (14%) [Table - 2]. Gallbladder wall congestion and thickness was more in symptomatic patients, but the mucosal charges were similar in both symptomatic and asymptomatic gallbladders. The number and nature of stones did not have any bearing on the gross changes. Microscopic examination Normal epithelium was seen in 13 specimens (9%). Epithelial hyperplasia was observed in 83 (69%), antral metaplasia in 23 (16.5%), intestinal metaplasia in 22 (15.5%), dysplasia in 12 (8.5%) and carcinoma in situ in 1 specimen (0.7%). Fibrosis and ulceration was found in 26 specimens (19%). Out of 83 specimens with epithelial hyperplasia, associated antral metaplasia was present in 13 (16%), intestinal metaplasia in 16 (19%) and dysplasia in 5 specimens (6%). Three patents (4%) had features of both antral and intestinal metaplasia with hyperplasia and 1 (1-5%) had hyperplasia with both types of metaplasia and dysplasia. Only 1 case of carcinoma in situ was found out of 140 specimens (0.7%). No case of invasive carcinoma of gallbladder was detected amongst the 140 patients operated for cholelithiasis [Table - 3]. These histological changes were similar in patients with symptomatic as well as asymptomatic gallstones. There was no difference in the epithelial changes with respect to either number or character of the gallstones. Twenty cases of invasive gallbladder cancer were also included in the study. In these specimens, the mucosa adjacent to the carcinomatous area was studied. Carcinoma in situ was found in 8 (40%), dysplasia in 5 (25%), hyperplasia in 4 (20%), antral metaplasia in 4 (20%) and intestinal metaplasia in 2 (10%) specimens [Table - 4]. Stones were found in 18 of these 20 gallbladder cancer specimen. Discussion Carcinoma of the gallbladder is the commonest malignancy of the biliary tract. The incidence of the disease in India is 2.3 and 1.01 per 100,000 in female and male population respectively. It is 10 times more frequent in North compared to South India.[3] Gallstones appear to be the most important risk factor, being reported in 70-98% cases of gallbladder cancer, a far higher prevalence than that in age-matched general population.[4] Autopsy studies indicate that only 1-4% of patients with cholelithiasis develop cancer compared to less than 0.2% of those not containing stones.[5] Among asymptomatic gallstone patients followed up for 10-25 years, fewer than 1% developed cancer. Moreover, if stones on chronic inflammation were to be incriminated for cancer formation, then one would expect a higher incidence of squamous cell carcinoma instead of adenocarcinoma. Thus, clinical data does not establish a definite causative role for gallstones in the development of carcinoma although the association is sufficiently frequent to suggest common antecedents or at least a facilitative role. Cholelithiasis produces a series of epithelial pathological changes which could be precursor lesions of gallbladder cancer. These changes include hyperplasia, dysplasia and metaplasia. Epithelial hyperplasia is the most frequent change and was found in 60% of our gallbladder specimens with stone disease. In 20%, hyperplasia was associated with metaplasia and in 6% with dysplasia. Albores - Saavedra et al suggest that a small number of hyperplasia of the gallbladder evolves towards atypical hyperplasia and that this may progress to in situ carcinoma which finally becomes invasive carcinoma.[6] Metaplasia of the antral and intestinal variety is frequently seen in gallbladders containing stones. We found about 16% of each, antral and intestinal metaplasia, in our specimens while others have reported the incidence of antral metaplasia in 50 to 100% of their cases with lithiasis.[7],[8] The frequency and severity of mucous gland hyperplasia and metaplasia was also found to increase with age and was more commonly observed in patients above 40 years of age. It is widely accepted that metaplastic epithelium is more susceptible to malignant transformation than normal. Yamamoto et al have proposed that there may be two histogenetic pathways for gallbladder cancer, one path derived from normal epithelium and the other from metaplastic epithelium.[9] Epithelial dysplasia was found in 8.5% of gallbladder specimens. Among the 20 cases of invasive carcinoma, dysplasia was present in the adjacent mucosa in 25%. Martinez et al reported low-grade dysplasia in 40% and high-grade in 16% of cases with lithiasis. Others have reported the incidence of dysplasia in 2.2% of cholelithiasis specimens and 42% in the mucosa adjacent to invasive carcinoma.[8] Reasons for the wide discrepancy in the reported incidence of dysplasia could be the number of sections examined and the criteria for histological diagnosis used in various studies. Significantly, our study could not show any difference in histological changes based on either the numbers or nature of the gallstones. Similar results were also reported by Martinez et al,[8] who also could not demonstrate a relationship between the type and numbers of gallstones to the epithelial changes occurring in the gallbladder. Carcinoma in situ was found in only 1 out of 140 cholelithiasis specimens (0.7%). Among invasive carcinoma specimens, carcinoma in situ was found in the adjacent mucosa in 8 out of 20 specimens (40%). Duarte et al[10] found carcinoma in situ in 3.5% of cholelithiasis specimens. They also observed carcinoma in situ in the mucosa adjacent to invasive carcinoma in 79% of cases and 52.9% of autopsy cases. The great majority of in situ carcinomas is grossly indistinguishable from cholecystitis and can easily be overlooked on macroscopic examination. The thickness of the gallbladder wall may be normal or minimally thickened. The mucosa may appear granular, slightly nodular, plaque-like or trabulated. Thus the pathologist may have no definite guide as to where to cut the representative section and the incidence of in situ carcinoma could be greatly underestimated. Albores - Saavedra et al[2] found a 10-year difference in the mean age of patients with carcinoma in situ and those having invasive carcinoma. It gives support to the idea that carcinoma in situ grows slowly and is a precursor lesion of invasive gallbladder cancer. According to Duarte et al, a single random histological section will detect less than one-third of hyperplasias, dysplasias and carcinomas in situ. Thus our study could be missing two-thirds of these lesions. The malignant potential of these conditions in gallbladders is uncertain, but the probability of malignant transformation would progressively increase from hyperplasia to metaplasia to dysplasia to carcinoma in situ. Management of asymptomatic gallstones is still a controversial issue and most surgeons feel that these patients can safely be followed up without cholecystectomy. However, Eastern UP and the Indo-Gangetic belt have amongst the highest incidence of gallbladder carcinoma in the world.[1] We have shown conclusively that even asymptomatic gallstones can produce a series of epithelial pathological changes in the gallbladder mucosa which could be precursor lesions for gallbladder carcinoma. This could be especially relevant in younger patients with asymptomatic gallstones who live in the Indo-Gangetic belt. Thus our work supports the contention that cholecystectomy should be offered to all asymptomatic gallstone patients, especially if they are less than 60 years of age and are living in a high-incidence area for gallbladder carcinoma. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06058t1.jpg] [is06058t4.jpg] [is06058t2.jpg] [is06058t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}