 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
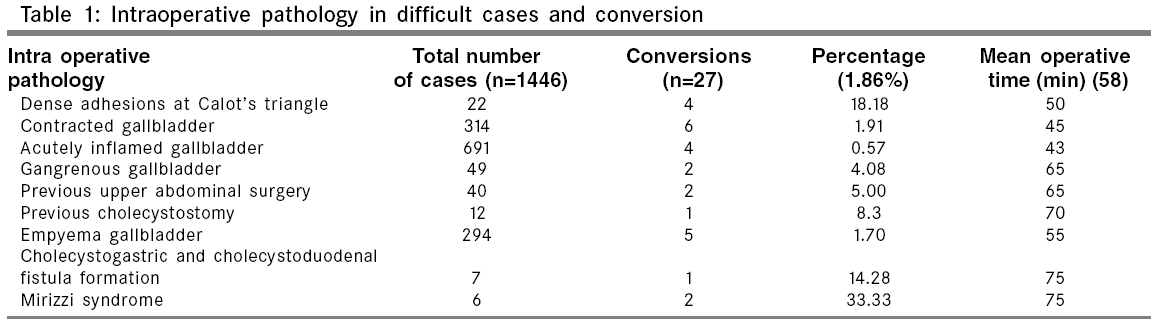
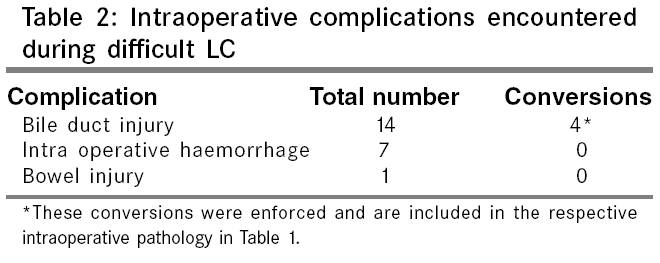
Indian Journal of Surgery, Vol. 68, No. 4, July-August, 2006, pp. 205-208 Original Article Difficult laparoscopic cholecystectomy: A large series from north India Singh Kuldip, Ohri Ashish Department of Surgery, Dayanand Medical College and Hospital, Ludhiana Correspondence Address:Singh Kuldip, 508 L, Model Town, Ludhiana - 141 002, Punjab, India. E-mail: drkkanda@rediffmail.com Code Number: is06059 Abstract Background: Laparoscopic cholecystectomy (LC) has become the gold standard for gallstone disease. We present one of the largest series of LC from the high prevalence area of gallstone disease.Aim: To analyze the single-center experience with respect to conversion rate and complication rate. Settings and Design: Retrospective observational study. Materials and Methods : Data of all the patients who were operated between May 1992 and July 2005 was collected retrospectively and difficult cases were identified out of them based on the intraoperative pathology. These cases were analyzed in relation to conversion to open surgery and complication rate. Results : LC was performed in 6,380 patients at our center. Based on the criteria selected on the intraoperative pathology, 1,446 (22.66%) cases were identified as difficult cases. Laparoscopy had to be abandoned and the procedure was converted to conventional surgery in 27 patients with a conversion rate of 1.86% (n=27) of the difficult cases and 0.42% (n=27) of the total LCs done. All the conversions were in the difficult group. The most common intraoperative complication was bile duct injury (n=14) (0.96%), which led to four conversions. Conclusions : From our experience, we emphasize that the experience of the surgeon and meticulous surgical technique are the most important factors to achieve a low complication rate. Keywords: Laparoscopic cholecystectomy, complication, conversion Introduction Cholecystectomy was established as the surgical treatment for cholelithiasis in 1882, when Carl Johann August Langenbuch performed the first cholecystectomy in a 43-year-old man who was suffering from gallstone disease for 16 years.[1] Open cholecystectomy (OC) enjoyed the status of gold standard treatment for cholelithiasis till the late 1980s, when Philip Mouret from France performed the first human laparoscopic cholecystectomy (LC) in 1987.[2] Just after 2 years of its birth, the first LC was done in India by T. E. Udwadia in 1989. Soon due to its remarkable advantages over OC - i.e., less postoperative pain, early recovery and decreased length of hospital stay - LC became the gold standard for the treatment of symptomatic gallstone disease. In the early years of LC, pregnancy, acute cholecystitis, gangrenous gallbladder, empyema, cholecystitis with cirrhosis, pancreatitis and Mirizzi syndrome were considered absolute contraindications for LC. As the advances in laparoscopic skills have evolved, the indications have expanded to make these traditional contraindications only relative.[3] The gallstone disease is more common in this part of the world and a large number of cases present in the advanced stage of disease. We, being the pioneers of LC in the northern India, have one of the largest series to present our experience in difficult LC from the region. Materials and methods We started performing LC in 1992. Data of all the patients who were operated between May 1992 and July 2005 was collected retrospectively and difficult cases were identified out of them and analyzed based on intraoperative pathology. Ultrasonography (USG) remained the investigation for the preoperative diagnosis of gallstone disease.[4] Our policy was to attempt LC in all the patients who required cholecystectomy and were fit for laparoscopy. Patients having absolute contraindications to laparoscopy, like cardiovascular and severe pulmonary disease, were not included. Indications for LC were acute cholecystitis, chronic cholecystitis, biliary colic, symptomatic gallbladder polyp, gallstone pancreatitis, porcelain gall bladder and asymptomatic large gallstone (>2 cm). Choledocholithiasis was suspected preoperatively, based on raised serum levels of alkaline phosphatase, history of cholangitis, stone visible in common bile duct (CBD) on USG or dilated CBD. CBD was cleared in these patients with endoscopic retrograde cholangiography and then LC was undertaken. Patients who failed endoscopic clearance of CBD stones were subjected to OC with CBD exploration and were not included in the study. Out of all the cases that underwent LC, difficult cases were identified based on intraoperative pathology. We defined difficult LC as 1) dense adhesions at the triangle of calot (frozen triangle of calot prohibiting laparoscopic dissection without significant risk), 2) chronic cholecystitis with contracted and fibrotic gallbladder, 3) previous upper abdominal surgery with adhesions to the anterior abdominal wall, 4) gangrenous gallbladder, 5) acutely inflamed gallbladder, 6) empyema of the gallbladder, 7) cholecystogastric or cholecystoduodenal fistula, 8) previous cholecystostomy and 9) Mirizzi syndrome. These cases were analyzed in relation to conversion to open surgery and complication rate. Results From May 1992 to July 2005, LC was performed in 6,380 patients at our center, out of which 2,250 were males and 4,130 were females, with an average age of 49 years (range 22-84 years). Based on the criteria selected on the basis of intraoperative pathology, 1,446 (22.66%) cases were identified as difficult cases. LC was successfully completed in 6,353 patients with a success rate of 99.58% (n=6353). Laparoscopy had to be abandoned and the procedure was converted to conventional surgery in 27 patients with a conversion rate of 1.86% (n=27) of the difficult cases and 0.42% (n=27) of the total LCs done. All the conversions were in the difficult group. Total number of conversions and their percentage in each group of patients is detailed in [Table - 1]. Only four conversions were done inevitably due to intraoperative bile duct injury [Table - 2]. Two patients had small contracted gallbladder and while dissecting in the triangle of calot, common hepatic duct suffered a lateral injury (Strassberg type D). One patient had frozen calot′s triangle and lateral injury was accidentally done to the common hepatic duct as in the previous cases (Strassberg type D). One accidental linear tear occurred in the anterior wall of the common bile duct while dissecting in the triangle of calot in a patient having Mirizzi syndrome (Strassberg type D). All the injuries to the bile ducts were identified intraoperatively on table. The procedure was converted to conventional surgery and repair was done over a T-tube. It has been our policy to keep a drain after LC for 24 h. Ten patients had increased postoperative bile leak for more than 24 h, which stopped within a period of 1 week. However, the source of bile leak could not be identified. In five patients, endoscopic retrograde cholangiography and stenting of CBD was done to decrease the bile leak, but the source of bile leak could not be located. In the other five, bile leak stopped spontaneously. We categorize them as minor leak from the gallbladder bed (Strassberg type A). We encountered intraoperative hemorrhage in only seven cases, but none had to be converted, for the same reason and LC was successfully completed in all the patients, taking the help of the gauze piece and suction to control the hemorrhage laparoscopically [Table - 2]. Bowel injury occurred accidentally in one case at the time of insertion of the veress needle, but the same did not warrant conversion and the primary repair of the small intestine was done laparoscopically [Table - 2]. It was our policy to administer NSAIDs postoperatively for 48 h, unless contraindicated, to provide adequate analgesia and antibiotic cover was provided with second-generation cephalosporin (cefuroxime, 1.5 gm 1 h before induction and 750 mg eight hourly postoperatively) for 24 h. The mean hospital stay for the patients was 1.5 days. Only three patients developed surgical site infection, which was cured with daily dressings; however, we did not encounter any case of port site hernia. There was no mortality. Age, sex, previous abdominal surgery and, most importantly, surgeon′s experience were found as important determinants of successful outcome. Discussion The first account of gallstones was given in 1420 by a pathologist Antonio Benevieni, in a woman who died with abdominal pain.[5] First interaction of surgery and gallstones dates back to 1687, when Stal Pert Von Der Wiel, while operating a patient with purulent peritonitis, accidentally found gallstones.[6] With the passage of time, first, open cholecystectomy; and then, laparoscopic cholecystectomy were established as the gold standard for the treatment of gallstone disease. Ascending along the learning curve, the incidence of complications during LC has been reduced markedly up to the level of 1-6%;[7],[8],[9] however, the incidence is higher than during open cholecystectomy and efforts are being made to reduce this further.[10] In our series, we had a conversion rate of 1.86% of the 1,446 difficult cholecystectomies and 0.42% of the total LCs performed at our center, which is lower than the incidence reported in literature, which varies from 2% to as high as 22%.[10],[11],[12] Our most common intraoperative pathology for which the conversion had to be done was Mirizzi syndrome - two out of six (33.33%). Mirizzi syndrome is a rare complication of longstanding gallstone disease, which has been reported to have a high conversion rate[13],[14] and high incidence of bile duct injury. One conversion out of the two was enforced due to the accidental linear injury in the anterior wall of the CBD, which was managed in the same sitting; and in the second patient, anatomy could not be defined in the calot′s triangle. We could not diagnose Mirizzi syndrome in any of our patients preoperatively as the clinical presentation was not different from acute cholecystitis and USG could not pick up the pathology. We are in agreement with Curet et al and Antonios et al that preoperative diagnosis of Mirizzi syndrome is not required for a successful outcome.[14],[15] Further, retrospectively we analyzed that we could have avoided these conversions by opting for laparoscopic subtotal cholecystectomy.[16] The second most common intraoperative pathology leading to conversion was frozen triangle of calot- 18.18%. Dense adhesions and fibrosis in the calot′s triangle make the dissection very difficult and anatomy unclear, causing a high level of difficulty. We had to convert 18.18 % of the patients having dense adhesions to open surgery, which is lower than reported in literature.[10],[17] Conversion rate was 1.91% (6 out of 314) in patients having chronic cholecystitis, which is much less than the earlier reported series of Chahin (5.5%) and Singer (2.8%).[12],[18] Acute cholecystitis makes the tissues friable and difficult to hold by the instruments, along with the increased vascularity, which raises the level of difficulty in acute setting. Many series have reported in favor of the early intervention in cases of acute cholecystitis (< 48 h) rather than intervening later in the course.[19],[20] Our policy was to intervene in the cases presenting within 72 h of onset of symptoms and our conversion rate in the setting of acute cholecystitis (0.57%) is much lower than reported in many series.[11],[12],[19],[21] We contradict the statement/conclusion/inference/opinion of Knight et al that timing of urgent LC does not influence the conversion rate.[22] Knight et al had reported a conversion rate of 12%, which is much higher than reported in literature. We advocate that once there is marked tenderness in the right hypochondrium with symptoms of more than 72 h duration, invariably one should defer surgery. Even in some unprecedented situations, when we come across an inflamed and fiery gallbladder, our policy has been to take out the scope and defer the surgery till 4 weeks. By doing so, we do not lose anything but give an advantage of the minimal access surgery to the patient. Double admission of the patient might have an economic effect in the developed countries, but higher rates of conversion also entails higher patient morbidity and higher operating costs. Gangrenous gallbladder is a grave pathology that makes tissues so friable that gallbladder may perforate even with cautious handling, making the operation difficult. Many authors have reported a conversion rate varying from 16% (by Kiviluoto et al ) to 40% (by Elder).[23],[24] We could achieve a lower conversion rate of 4.08% in cases with gangrenous gallbladder by virtue of the skills and large experience. We could successfully complete LC in most of the patients having previous upper abdominal surgery - 38 out of 40 - with a conversion rate of 5.00%, which is lower than reported in literature.[3] Cholecystoenteric fistula, although making LC difficult, no longer remains a contraindication to laparoscopy. We could complete five out of seven cases of cholecystoenteric fistula laparoscopically. We concur with Francesco et al that when the surgeon is skilled in laparoscopic operative techniques such as duodenal mobilization and intracorporeal suturing and knotting, cholecystoenteric fistulas are not a contraindication to laparoscopy.[25] Another common pathology that is encountered frequently in the developing countries is empyema of the gallbladder, which signifies the advanced stage of acute inflammation of gallbladder. The preoperative risk factors for the condition include duration of complaints more than 48 h and a palpable gallbladder - a combination indicating advanced gallbladder disease.[24] Various authors have reported a very high rate of conversion associated with this pathology, ranging from 12.5 to 83%.[24],[26] We had a conversion rate of 1.7% in cases having empyema of gallbladder, which is much lower than reported in literature. We attribute the low rate of conversion to the fact that we follow the basic rules of surgical technique strictly - like use of veress needle, adequate vision, minimal use of electrocautery at the triangle of calot, displaying the structures at the triangle of calot before clipping, adequate traction in proper direction, use of gauge dissection in difficult cases and reconfirming the anatomy from time to time. We have been operating in a single center with the same Chief Operating Surgeon, which played a major role in achieving the low conversion rate as has been reported.[10],[27] The most common intraoperative complication was bile duct injury (n=14) (0.96%), which led to four conversions. The incidence of bile duct injury in our experience is 0.96% with a conversion rate of 0.28%, which is lower than that of reported literature.[9],[10],[11],[12] The other intraoperative complications like intraoperative hemorrhage (n=7) and bowel injury with the veress needle (n=1) were managed successfully laparoscopically and did not warrant conversion to open surgery. Conclusion From our experience, we emphasize that the experience of the surgeon and meticulous surgical technique are the most important factors to achieve a low complication rate. One should avoid any kind of misadventure in case a complication occurs and threshold for conversion should be kept on the lower side.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06059t2.jpg] [is06059t1.jpg] |
| |||||||||

{kind=link}
{kind=link}