 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
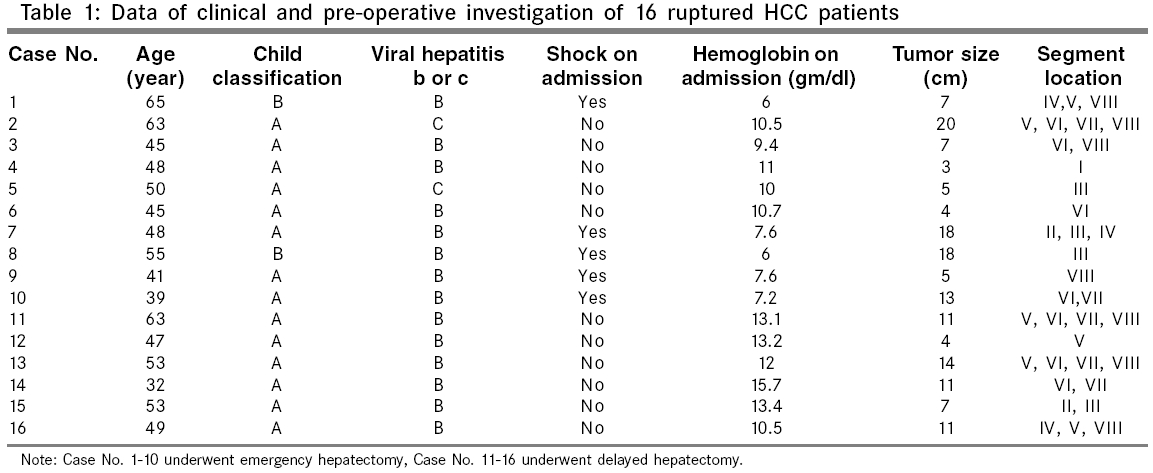
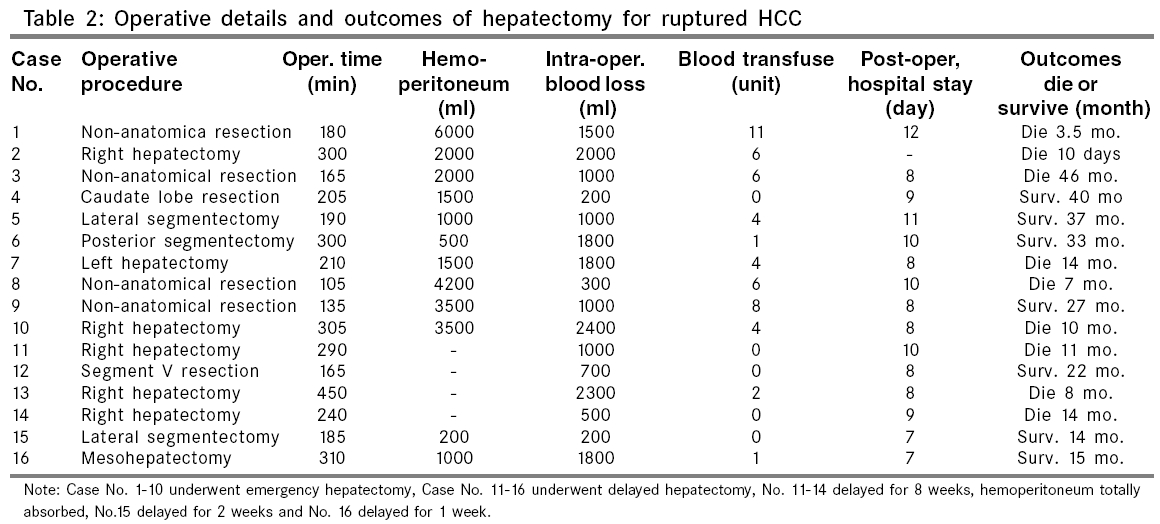
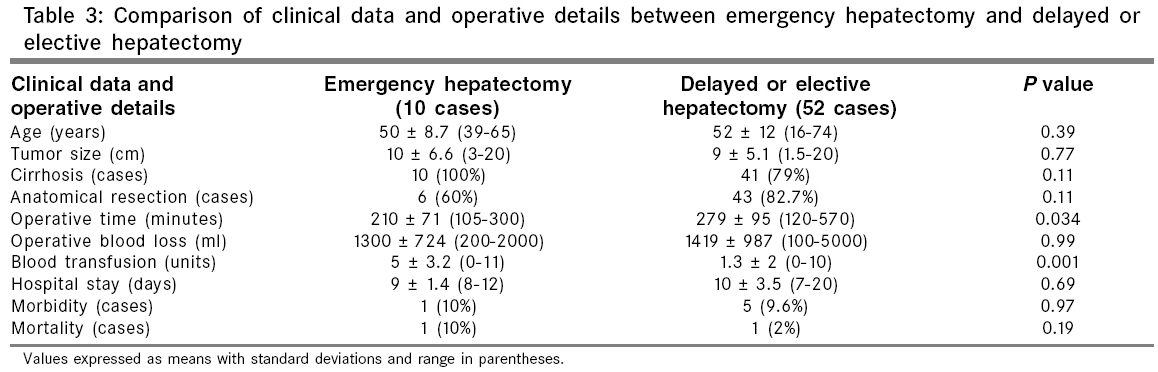
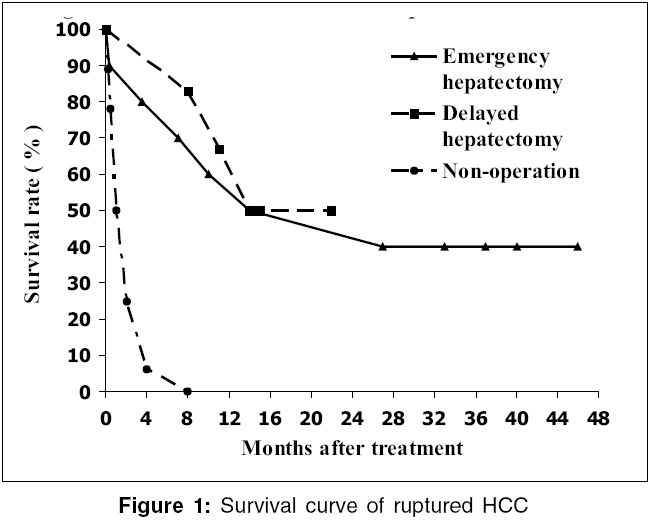
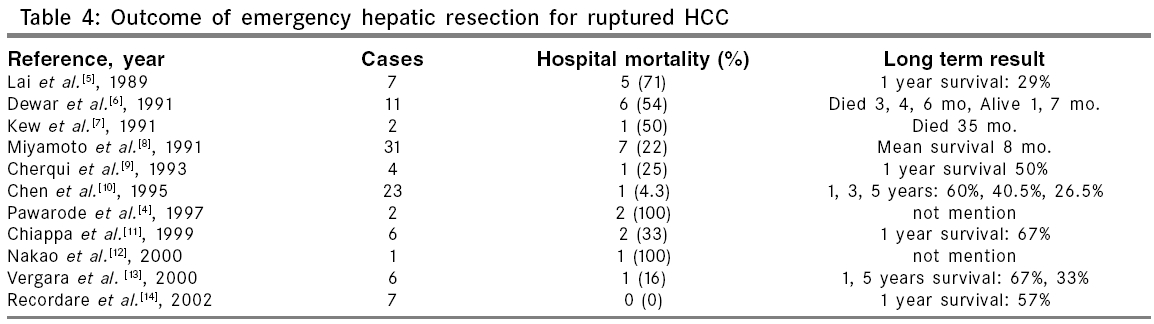
Indian Journal of Surgery, Vol. 68, No. 4, July-August, 2006, pp. 209-215 Original Article Delayed versus emergency hepatectomy for ruptured hepatocellular carcinoma Anon Chotirosniramit Department of Surgery, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand - 50200 Correspondence Address:Chotirosniramit Anon, Department of Surgery, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand - 50200. E-mail: achotiro@hotmail.com Code Number: is06060 Abstract Background and Aims : Ruptured hepatocellular carcinoma (HCC) is a life-threatening complication of HCC. Delayed hepatectomy after successful hemostasis or emergency hepatectomy is the controversial issue of the treatment for resectable ruptured HCC. The aim of this study was to evaluate outcomes of these procedures for ruptured HCC.Materials and Methods : From 2001 to 2005, hepatectomy for HCC was performed by the author on 62 patients, Of these, 16 patients had ruptured HCC. Emergency hepatectomy was performed in 10 patients and delayed hepatectomy in the remaining 6. Clinical data and outcomes following hepatectomy for ruptured HCC were reviewed and analyzed retrospectively. Results : In emergency hepatectomy group, there was one complication of transient gastric atony and one of postoperative death from massive variceal bleeding. A 1-year survival rate was 60% with a mean survival of 22 months. No postoperative complication and death was found in delayed hepatectomy patients but three died in 8, 11 and 14 months due to lung metastasis. A 1-year survival rate was 67% with a mean survival of 14 months. No statistically significant difference in morbidity and mortality rate was found between the emergency hepatectomy group and delayed or elective hepatectomy group. There was no significant difference in overall survival between emergency and delayed hepatectomy groups. Conclusion : Emergency hepatectomy may be a life-saving procedure for resectable ruptured HCC patients who have massive and continuous bleeding, particularly if emergency transarterial embolization is not available . To avoid difficult delayed hepatectomy and with concern for the rapid progression of cancer, delayed hepatectomy should be performed as soon as possible. Keywords: Delayed hepatectomy, emergency hepatectomy, hepatocellular carcinoma, ruptured hepatocellular carcinoma Ruptured hepatocellular carcinoma (HCC) is a ′not uncommon′ life-threatening complication, which has been reported to occur in 9-14.5% of patients with HCC.[1],[2],[3],[4] Current methods used to treat ruptured HCC include both surgical interventions such as emergency and delayed hepatectomy and nonsurgical means such as transcatheter arterial embolization (TAE) and conservative treatment. The aim of treatment is to achieve hemostasis and remove the tumor as early as possible. Although emergency hepatectomy has been proposed as the ideal treatment for resectable ruptured HCC, it unfortunately carries very high mortality rate according to previously published reports.[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] Given the high mortality risk associated with this procedure, some authors have recommended TAE for hemostasis, followed by delayed hepatectomy for resectable ruptured HCC.[1],[15] However, in most hospitals in Thailand, emergency TAE is not available or feasible. Patients with hypovolemic shock from ongoing massive bleeding may die within a few hours after admission. Emergency hepatectomy may save lives. Personal experience with hepatectomy for ruptured HCC is presented. Materials and Methods Patients From May 2001 to July 2005, hepatectomy was performed by the author on 163 patients. Of these, 17 patients had benign liver disease and 116 patients had malignant liver disease, including 62 having HCC; 73, cholangiocarcinoma; 6, liver metastasis; and 5, other primary liver cancers. Among the 62 HCC patients, 16 cases were diagnosed as ruptured HCC. Of these, 10 patients underwent emergency hepatectomy and 6 underwent delayed hepatectomy. The clinical data of all resectable HCC patients and outcomes following hepatectomy for ruptured HCC were reviewed and analyzed retrospectively. Almost all ruptured HCC patients were diagnosed pre-operatively based on clinical manifestations, ultrasonography, abdominal computed tomography and/or abdominal paracentesis that showed the liver tumors with hemoperitoneum. After diagnosis, the patients were resuscitated with rapid intravenous fluid administration for stabilizing the blood pressure. Complete blood count, coagulogram and liver function test were determined. Indocyanine green clearance determination was not available in this hospital, so hepatic functional reserve was determined by Child-Pugh score. In the author′s policy, emergency hepatectomy was pursued in all ruptured HCC patients who were first diagnosed and deemed to have resectable tumors and good hepatic functional reserve on the basis of imaging studies and Child-Pugh Classification. Resectability of the tumor was assessed by computed tomographic scan that showed unilateral lobar involvement by tumor without main portal vein thrombosis. Hepatic functional reserve of the patients should be Child-Pugh class A or B. Ten patients were selected to undergo emergency hepatectomy. All 6 patients in the delayed hepatectomy group were referred from other hospitals following successful conservative treatment, including one who had received TAE for hemostasis from a hospital in Bangkok. The interval of delayed hepatectomy depended on the referral duration and the schedule of elective operation. In the same period, there were 18 cases of unresectable ruptured HCC receiving various methods of treatment, such as conservative treatment, TAE, perihepatic packing and hepatic arterial ligation. Patients with unresectable terminal disease, including those with cachexia, liver failure and extensive involvement of both hepatic lobes received conservative treatment. In patients with unresectable disease not defined as terminal, TAE was the treatment of choice if active bleeding was presented. If emergency TAE was not available, nonresectional surgical hemostasis such as perihepatic packing or hepatic arterial ligation was performed. Operative procedures Emergency hepatectomy was defined as hepatectomy within 24 h after diagnosis of ruptured HCC. Delayed hepatectomy was defined as hepatectomy within days or weeks after diagnosis. The patient was placed on the operating table with the right side elevated about 30°, suspending the right arm from a soft sling attached to the bar in flexion of the elbow and shoulder joint. Long right subcostal incision was used to open abdomen. After entering peritoneal cavity, blood was aspirated to estimate hemoperitoneum. If active bleeding was present, swab packing and/or intermittent hepatic inflow occlusion were used to stop bleeding temporarily. The selection of types of hepatic resection was dependent on location of the tumors. Anatomical resection of the segment or lobe where the tumor was located was preferred. In some cases in which the tumors protruded as exophytic tumors, non-anatomical resection was performed. Statistical analysis Statistical analysis was performed by the Mann-Whitney U test to compare continuous variables and the chi-square test was used to compare discrete variables. The Kaplan-Meier method was used to estimate overall survival. Statistically significant differences in the survival rates were determined with the log-rank test. Statistical significance was defined as a P value of less than 0.05. Statistical calculations were performed using SPSS software (SPSS Inc, Chicago, IL). Results All 16 resectable ruptured HCC patients except one were male with a mean age of 49 ± 8.9 (SD) years (range 32-65 years). Fourteen patients had cirrhosis due to hepatitis B virus, while 2 had cirrhosis secondary to hepatitis C virus. Severity of liver dysfunction was evaluated with the Child-Pugh classification. Fourteen patients were Child-Pugh class A and 2 were Child-Pugh class B. Acute abdominal pain was the first symptom in all cases. One patient was initially misdiagnosed as having a perforated peptic ulcer prior to surgery. Ten of the 16 patients had alpha-fetoprotein levels that were elevated to more than 20 ng/ml. The mean tumor size was 9.9 ± 5.5 cm (range 3-20 cm). Data of clinical and pre-operative investigation are summarized in [Table - 1]. Surgical outcomes and operative details regarding operative procedures, operative time, volume of hemoperitoneum, intra-operative blood loss, unit of blood transfusion and postoperative hospital stay are summarized in [Table - 2]. In the emergency hepatectomy group, 5 of the 10 patients had clinical shock during initial admission, with a hemoglobin level of less than 8 gm/dl. Rapid fluid administration could restore the blood pressure of all cases. Emergency operative procedures included two right hepatectomy, one left hepatectomy, one lateral segmentectomy, one posterior segmentectomy, one caudate lobe resection and four non-anatomical resections. During the operation, the ruptured HCC had active bleeding in 7 of 10 cases and 5 of them required intermittent hepatic inflow occlusion, with an average time of 19 min. The mean volume of hemoperitoneum (aspirated blood content before hepatectomy) was 2,570 ± 1,694 ml (range 500-6,000 ml). All patients except one received blood transfusions. The mean operative time was 210 ± 71 min (range 105-300). The mean intra-operative blood loss (estimated blood loss during hepatectomy) was 1300 ± 724 ml (range 200-2000). The mean volume of blood transfusion was 5 ± 3.2 units (range 0-11). The mean postoperative hospital stay was 9 ± 1.4 days (range 8-12). There was 1 morbidity patient, who underwent lateral segmentectomy including excision of hepatogastric ligament that contained the vagus nerve along with fragments of ruptured tumor. As a result, this patient developed transient gastric atony for 8 days after the operation. There was 1 mortality patient, who had initially been misdiagnosed as a peptic ulcer perforation but was later found at surgery to have hemoperitoneum due to a ruptured HCC. Despite an additional 2,000 ml blood loss during right hepatectomy, the patient was stable in the postoperative period with 6 units of blood transfusion. Unfortunately, the patient developed massive esophageal variceal bleeding with hypovolemic shock and died on postoperative day 10. Regarding surgical outcomes, 4 patients died due to hepatic failure from recurrent disease in remaining liver in 3.5, 7, 10 and 14 months following the operation. One patient died due to brain metastasis 46 months after surgery. Four patients were still alive at the time of this study - at 27, 33, 37 and 40 months following the operation. Two survival patients had recurrent - 1 had recurrent disease in the residual hepatic parenchyma and received transcatheter arterial chemoembolization and percutaneous ethanol injection; the other case had recurrent disease at the chest wall and received chest wall resection. Two patients had no recurrent disease at 27 and 40 months of follow-up. The 1 and 2 year survival rates were 60 and 50% respectively, with a mean survival of 22 months. There were three patients in this case series who had advanced ruptured HCC and were selected for emergency hepatectomy. In case no.1, the patient had profound shock and marked abdominal distension due to 6 liters of hemoperitoneum. A computed tomographic scan showed cirrhotic liver, with a 7 cm ruptured HCC involved in anterior and medial segment, with massive hemoperitoneum and extravasation of the contrast media. After non-anatomical resection, the patient was discharged on postoperative day 12 without complication. The patient died 14 weeks later due to progression of the residual disease. In case no. 5, a computed tomography scan showed a 5 cm ruptured HCC at the lateral segment and 3 HCC nodules, 1-2 cm in diameter at the right lobe. Lateral segmentectomy was performed. After recovery from the postoperative period, three residual nodules were treated with percutaneous ethanol injection and transarterial chemoembolization. The patient is alive and well 3 years later. In case no. 8, the patient developed shock, with hemoglobin at 6 gm/dl. A computed tomographic scan showed multiple HCC involved in both lobes. The ruptured HCC was located at Segment III as a protrusion mass with an 18 cm diameter. Emergency non-anatomical resection was performed to save the patient′s life. Hemoperitoneum and further intra-operative blood loss were 4,200 ml and 300 ml respectively. The patient recovered well and was discharged 10 days after the operation. He died due to his advanced disease 7 months later. In the six patients undergoing delayed hepatectomy, the operation was postponed for 1 week after rupture in one case, 2 weeks in one case and 8 weeks in four cases. The procedures included three right hepatectomies, one segment V resection, one lateral segmentectomy and one mesohepatectomy. Peri-operative blood transfusion was required in two patients, one of whom received 1 unit, while the other received 2. All patients were discharged in 7-10 days after the operation without any complication. Although all had an uneventful postoperative recovery course, three patients developed lung metastasis very soon afterwards and died in 8, 11 and 14 months after diagnosis of the ruptured HCC. The remaining three patients survived in 14, 15 and 22 months after surgery. One had recurrent disease in the liver and received percutaneous ethanol injection. A 1-year survival rate was 67% with a mean survival of 14 months. Among 46 cases of HCC that underwent elective hepatectomy for nonruptured HCC in the same period, 5 cases developed postoperative complications including one of superficial surgical site infection, one of urinary tract infection, one of ascites and two of bile leakage. One postoperative death was due to liver failure. Clinical data and operative details were compared between the group receiving emergency hepatectomy for ruptured HCC and that receiving delayed hepatectomy for ruptured HCC or elective hepatectomy for nonruptured HCC in the same period [Table - 3]. There was no significant difference in age, tumor size, type of resection, prevalence of cirrhosis, intra-operative blood loss, duration of postoperative hospital stay, morbidity rate and mortality rate between both groups. The operative time of emergency hepatectomy was significantly shorter than that of delayed and elective hepatectomy ( P = 0.034), but significantly more blood transfusions were required in emergency hepatectomy ( P =0.001). There was no significant difference in overall survival between emergency hepatectomy group and delayed hepatectomy group ( P =0.81). The overall survival curve of the ruptured HCC patients is shown in [Figure - 1]. In the same period, 18 cases of unresectable ruptured HCC were managed by conservative treatment in 12 cases, TAE in 3 cases and nonresectional surgical hemostasis in 3 cases including one hepatic arterial ligation and two perihepatic packing. In the case receiving hepatic arterial ligation, the bleeding could be stopped but the patient died due to hepatic failure 1 month later. Two cases receiving perihepatic packing died due to hepatic failure 2 and 8 months later. In 12 cases receiving conservative treatment, 8 cases were documented as end-stage ruptured HCC that is defined by extensive involvement of the liver with poor hepatic functional reserve and all died within 1 month. The remaining 4 conservative treatment cases died within 4 months. In all 3 cases receiving TAE, bleeding could be stopped but 2 patients died 4 months later and one died 8 months later. A 1 month-survival rate of unresectable ruptured HCC was 50% and no patient survived for more than 8 months. Discussion In general, the prognosis of ruptured HCC is very poor. This complication may result in massive hemorrhage, shock, subsequent liver failure and death. Ruptured HCC may be a manifestation of the terminal stage of this disease. One large case series of 112 patients with ruptured HCC had an in-hospital mortality rate of 55 and 32% of them were classified as end-stage disease.[16] Another case series of 154 patients with ruptured HCC showed a 38% 30-day mortality rate.[1] Selection of patients for different treatments is individualized. It probably depends on extension of tumors, condition of the patients, availability of interventional radiologists and experience of surgeons. Conservative treatment is appropriate in terminal stage patients who have cachexia, liver failure, bilobar involvement and/or extrahepatic metastasis. The patients who have stable vital signs and minimal hemoperitoneum, without extravasation of the contrast media on imaging studies, may receive conservative treatment and subsequent definitive treatment such as hepatectomy or transarterial chemoembolization. The patients with unstable vital signs and continuous bleeding should be considered for immediate hemostasis. The least invasive method to stop bleeding of ruptured HCC is TAE, which has a success rate of about 83-100%.[1],[15] Even if hemostasis can be achieved, the hospital mortality rate would still be high and the prognosis is poor in unresectable patients.[1],[8],[15],[17],[18],[19],[20],[21],[22],[23] In the author′s experience, the prognosis of unresectable ruptured HCC is also extremely poor. All unresectable ruptured HCC patients died due to massive bleeding or liver failure within 8 months, with a 1 month mortality rate of 50%. Twelve of 18 cases had active bleeding; among these, TAE for hemostasis was resorted to in 3 cases, hepatic arterial ligation in 1 case, peri-hepatic packing in 2 cases and conservative treatment in 6 cases that were considered to be at end stage of malignancy. Bleeding in all cases who received TAE or nonresectional surgical hemostasis could be stopped. All end-stage HCC cases receiving conservative treatment died within 4 weeks. In patients with potentially resectable tumors, two options include emergency hepatectomy and delayed hepatectomy. Although emergency hepatectomy can achieve hemostasis quickly and concurrently remove resectable tumors, which seems to be the ideal treatment, several case series have demonstrated high postoperative mortality rates.[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] The causes of unsatisfactory results are- not knowing the exact details of hepatic functional reserve and coagulopathy-induced excessive blood loss during the operation. The mean hospital mortality rate in 11 reports during the years 1989 to 2004 (searched by PUBMED in the website of the National Library of Medicine with the keyword ruptured hepatocellular carcinoma ) was 27% (27 of 100 cases, range from 0-100%; [Table - 4]). [4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] To avoid postoperative complications and death, some authors have recommended delayed hepatectomy after successful hemostasis by conservative treatment or TAE, a method that has mortality rates comparable to those of elective hepatectomy for nonruptured HCC.[1],[8],[15],[19],[22],[24],[25],[26],[27],[28] However, this recommendation is on the basis of studies only as there are currently no randomized clinical trials reporting a comparison between these two approaches. A prospective randomized control study about treatments for ruptured HCC is difficult to conduct because the number of patients is limited and degree of bleeding varies. In Thailand, TAE is not available in most hospitals. Surgeons still play a role for hemostasis in ruptured HCC patients who have continuous bleeding. If the patients have pre-operative shock but good reserve of hepatic function and computed tomographic scan demonstrating extravasation of contrast media of the resectable ruptured HCC, emergency hepatectomy should be considered. In this case series, 5 of 10 cases had shock on admission, which was predicted to have massive and/or continuous bleeding, that showed as a large amount of hemoperitoneum. After stabilizing the patients with rapid intravenous fluid resuscitation, hemostasis with emergency hepatectomy was performed in all cases. With meticulous surgical technique and good intensive peri-operative care, the mortality and morbidity rate could be achieved as low as 10%. In the author′s experience, there was no statistically significant difference in intra-operative blood loss, morbidity rate and mortality rate between the emergency hepatectomy group and delayed or elective hepatectomy group and there was no postoperative liver failure in the emergency hepatectomy group. The long-term results of emergency hepatectomy showed a 2-year survival rate that was 50% with 46 months being the longest survival period. However, no statistical significant difference was found in overall survival between emergency and delayed hepatectomy. If the patients had stable vital signs and a computed tomographic scan showing minimal hemoperitoneum, conservative treatment with intravenous fluid and blood transfusion could be considered and followed with delayed hepatectomy for resectable tumors in later period. The disadvantage of delayed hepatectomy is the need to remove adjacent structures that are often involved or adherent as a result of the ruptured HCC. This makes the operation more difficult. In this series, en bloc resection of part of the diaphragm was performed with hepatectomy in three of six patients. Another risk of delayed hepatectomy is the often rapidly progressive nature of this malignancy and delayed treatment may increase the risk of metastasis, as occurred in three of four patients who underwent an operation 8 weeks after diagnosis. They developed lung metastasis very soon after the operation. Therefore, delayed hepatectomy should not be delayed for many weeks. The small size of HCC also can rupture if the tumor is located beneath the capsule of liver as a protrusion mass. In this case series, the tumor size was less than or equal to 5 cm in 5 of 16 cases but produced a large amount of hemoperitoneum - more than 1,000 ml - in 3 of 5 cases. The ruptured small HCC also had better prognosis than the ruptured large HCC. All cases survived more than 2 years and had no recurrent disease in 3 of them. In summary, although the prognosis of ruptured HCC is generally poor, long-term survival could be achieved in patients with resectable disease and good hepatic functional reserves. Emergency hepatectomy may be a life-saving procedure for ruptured resectable HCC patients who have massive and continuous bleeding. By experienced hepatic surgeons, emergency hepatectomy for this situation can be performed with low morbidity and mortality rate - the same as elective hepatectomy. If emergency transarterial embolization is not available for hemostasis, emergency hepatectomy is also an option for the treatment of resectable ruptured HCC. To avoid difficult delayed hepatectomy and with concern for the rapid progression of cancer, delayed hepatectomy should be performed as soon as possible. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06060t2.jpg] [is06060t1.jpg] [is06060t3.jpg] [is06060f1.jpg] [is06060t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}