 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
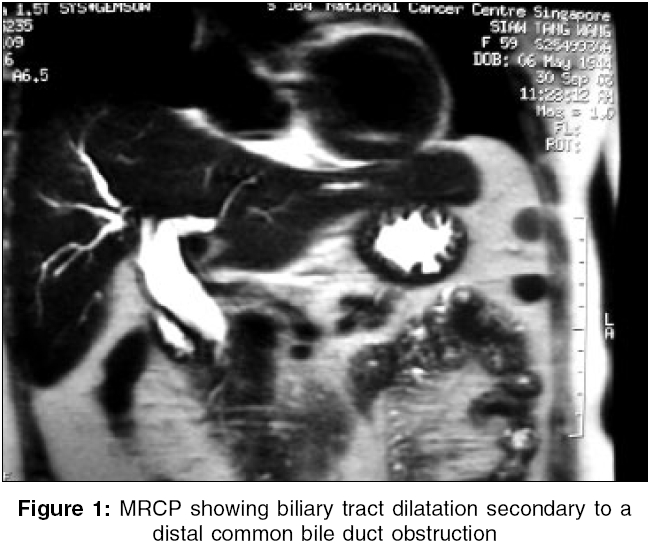
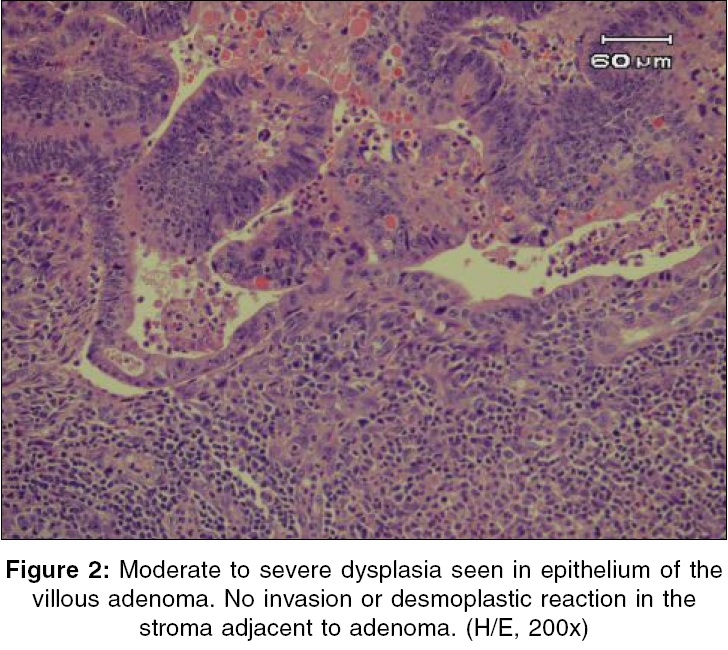
Indian Journal of Surgery, Vol. 68, No. 4, July-August, 2006, pp. 219-221 Case Report Biliary tract villous adenoma in a patient with gallbladder adenocarcinoma E-Shaun Goh, Kok-Yang Tan, Khoon-Hean Tay, Kent Mancer* Departments of General Surgery and *Pathology, Changi General Hospital, Singapore - 529 889 Correspondence Address:Kok-Yang Tan, Department of General Surgery, Changi General Hospital, 2 Simei Street 3, Singapore - 529 889. E-mail: kok_yang_tan@cgh.com.sg Code Number: is06062 Abstract We present a case of a 60-year-old lady who underwent cholecystectomy for T1N0M0 adenocarcinoma of the gallbladder in 1998. Six years later, she was found to have biliary tract obstruction, secondary to a distal common bile duct mass lesion. Radical resection was performed and histology revealed a villous adenoma of the bile duct. This case illustrates the need for biliary tree surveillance after diagnosis of gallbladder carcinoma. We also reviewed the literature on biliary tract villous adenomas.Keywords: Biliary cancer, biliary tract, gallbladder adenocarcinoma, villous adenoma Introduction Biliary tract villous adenoma is a rare entity. It is a benign epithelial lesion with a potential for malignancy. There is a low incidence in the duodenum and lower still in the biliary system compared to large bowel.[1] We report a case of biliary tract villous adenoma in a lady with a history of gallbladder adenocarcinoma.Case report A 60-year-old Chinese lady who underwent an elective cholecystectomy for T1N0M0 adenocarcinoma of the gallbladder in 1998. In September 2003, she developed obstructive jaundice. Magnetic resonance cholangiopancreatography (MRCP) revealed intrahepatic and extrahepatic biliary tract dilatation with distal ductal obstruction from possibly a malignant stricture [Figure - 1]. This was confirmed subsequently by endoscopic retrograde cholangiopancreatography (ERCP). A biliary stent was inserted therapeutically. Brush cytology revealed atypical cells. As biliary tract malignancy could not be excluded, Madam ST was advised to undergo an operation to explore the common bile duct. Intraoperatively, a mass lesion was discovered in the distal common bile duct and thus pancreatoduodenectomy was performed. The histological finding was that of a villous adenoma of the common bile duct. Mild dysplasia was noted within most of the adenoma with the presence of small areas of moderate to severe dysplasia [Figure - 2]. However, there was no malignancy present in the adenoma sample or within the margins of the common bile duct or the periductal tissue. Six lymph nodes were examined and found to be free from malignancy. The resected head of pancreas also did not harbor any malignancy. Postoperative recovery was uneventful except for prolonged ileus, which resolved. Discussion Biliary cancers are most common in Chile, Bolivia, Eastern Europe, Japan and India. Most occur without apparent etiology; however, obesity, chronic inflammation, Salmonella typhi infection and anatomical abnormalities have been implicated. There is also an obvious similarity between risk factors for gallbladder cancer and cholelithiasis. Mortality remains high, with a 5-year survival rate of 20 to 30%.[2] However, there is currently no evidence-based recommendation for primary prevention in average- to increased-risk populations. Villous adenomas of the biliary system are rare. Villous adenomas can occur at any part in the biliary tree. The presentation of these lesions is usually with symptoms similar to cholelithiasis, choledocholithiasis or cholecystitis. Acute pancreatitis and acute upper gastrointestinal bleeding[3] have also been described to be the result of these lesions. ERCP usually show a fixed filling defect at the level of tumor growth.[4] Endoscopic ultrasonography (EUS) has also been evaluated to adequately diagnose small lesions, but this may be superceded by intraductal ultrasonography.[5] This modality, which combines ERCP with a catheter probe sonography, has been proven to show higher sensitivity and specificity in diagnosis and staging of small periampullary tumors as compared with EUS or computed tomography.[5] Brush cytology is able to show cellular dysplasia[6] but has only been known to be 35% sensitive in diagnosis of malignancy.[6] Definitive diagnosis can only be made with histology, either by endoscopic means or open excision. Villous adenomas are a result of a mesenchymal proliferative dysplasia. They can be considered as a premalignant condition that eventually leads to adenocarcinomas via the adenoma-carcinoma sequence. Thus, adenomas of the biliary tract and gallbladder carry an increased risk of biliary cancers. Although biliary adenomas are benign, they do have characteristics that may give rise to cholangiocarcinomas.[7] In fact, clear cell cholangiocarcinomas have a similar immunohistochemical profile as that of atypical clear cell bile duct adenoma.[8] In this case, we postulate that there may have been a field change in Madam ST′s biliary system with resultant susceptibility to tumorigenesis. A report in Birmingham describes a similar occurrence of a gallbladder carcinoma and an incidental finding of a common bile duct adenoma 4 years later[9] may have described a similar circumstance. However, unlike in these two cases, most gallbladder cancer cases are detected at an advanced stage because of paucity of specific symptoms and thus have a short survival; thus, establishing linkage between these two entities is difficult. Treatment options are still being evaluated. For the time being, the general consensus is for radical resection of the villous adenoma.[10] This is in view of its likely potential for malignancy.[10] Biliary villous adenoma remains a rare but important entity due to their malignant potential. The detection of such lesions is a combination of clinical, radiographic and endoscopic features. Radical excision is still the preferred course of treatment. Definitive diagnosis is only from histology. Surveillance for biliary tract tumors is prudent after diagnosis of gallbladder carcinoma. However, sonographic screening for biliary adenomas in the general population is unlikely to be cost-efficient. The need for prevention of biliary tumors should be emphasized. The information on prevention of biliary cancers is likely to come from research addressing nutritional, metabolic, hormonal and genetic determinants of gallstones. Linking risk factors for the development of biliary stones should be able to clarify the origins of biliary tumors and develop effective preventive strategies. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06062f2.jpg] [is06062f1.jpg] |
| |||||||||

{kind=link}
{kind=link}