 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
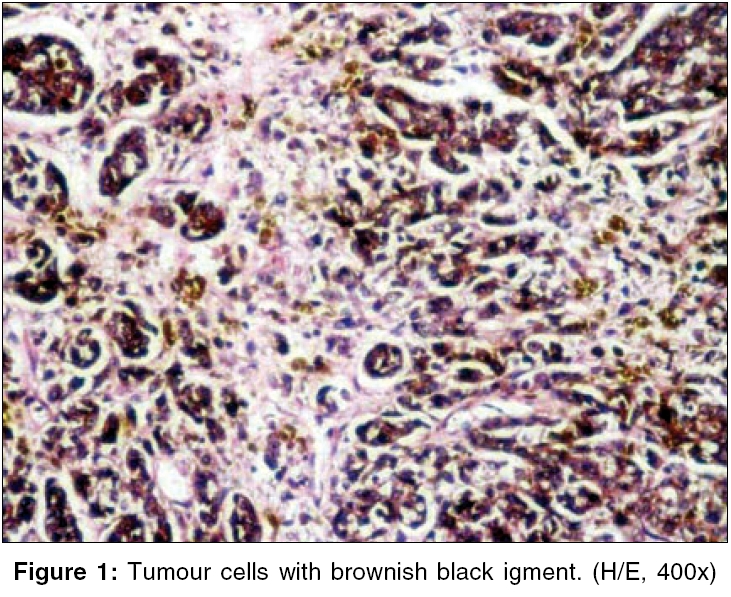
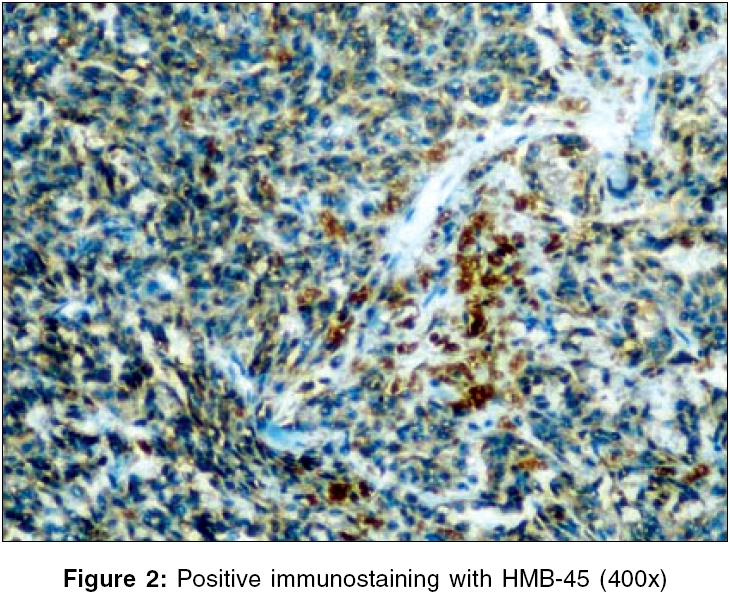
Indian Journal of Surgery, Vol. 68, No. 4, July-August, 2006, pp. 222-223 Case Report Small bowel metastasis of malignant melanoma S Radha, T Afroz, C Ratnakar*, Ashwin Kumar Reddy**, Satyanarayana G*** Dept of Pathology, Kamineni Hospitals, *Dept of Pathology, JIPMER Pondicherry, **Sri Srinivasa Hospital, ***Dept of Surgery, Kamineni Hospitals, Hyderabad, India Correspondence Address:S. Radha, Plot No.20, Road No.1, Alakapuri, Hyderabad - 500 035, India. E-mail: sradha_21@hotmail.com Code Number: is06063 Abstract Malignant melanoma shows an unusual predilection to metastasize to small intestine. A patient with metastatic spread of malignant melanoma to small intestine is reported. This patient was operated for intestinal obstruction. Metastatic melanoma should be suspected in patients with malignant melanoma who develop gastrointestinal symptoms.Keywords: Malignant melanoma, small bowel metastasis Introduction Metastatic spread from a tumor originating outside the abdomen rarely involves small intestine. Malignant melanoma shows an unusual predilection to small intestine with an incidence of 1.5-4.4%.[1] Malignant melanoma is the most common metastatic tumor involving the gastrointestinal tract.[2] Metastatic melanoma is more common than primary melanoma. Diagnosis is often delayed until the illness becomes an emergency for the patient due to complications of metastatic disease, such as intestinal hemorrhage, obstruction and perforation.[3] Any patient with a history of melanoma with abdominal symptoms must be assumed to have metastasis unless proved otherwise. We report a case of malignant melanoma metastasis to small bowel presenting with intestinal obstruction as the initial manifestation of his disease. Resection for obstruction and hemorrhage provides symptomatic relief in 72-92% of patients with a mortality of 5%.[4]Case Report A 55-year-old male presented with vomiting, distention of abdomen and constipation of 3 days duration. He was apparently normal before this. Physical examination revealed a moderately built adult male. He was febrile and there was distention of abdomen. Bowel sounds were absent. No mass was palpable. His laboratory values were normal. Plain X-ray of abdomen revealed multiple air fluid levels. Ultrasonography of abdomen revealed mild hepatomegaly and a hypodense lesion in the liver. As his clinical condition demanded, an emergency laparotomy was done. At laparotomy, there was an ileocolic intusussception with mesenteric lymphadenopathy. A segment of ileum and colon was resected. Resected specimen measured 38 cm. IIeum measured 26 cm. At 3 cm from the ileal end on the mucosal aspect, there was a solitary blackish nodular lesion of 1.5 x 1 cm. Cut surface of the lesion was blackish. Four lymph nodes were identified in the mesentery. Sections of nodular mass, on microscopic examination, revealed round to oval cells in sheets with indistinct cell borders. Nucleoli were prominent. There was abundant blackish brown pigment in the cytoplasm of these cells [Figure - 1]. This pigment was detected as melanin by Fontana Masson. Cells were positive with HMB 45 [Figure - 2] and S-100. Two nodes out of the four nodes revealed metastatic deposits. After a diagnosis of metastatic melanoma was given, a thorough clinical examination revealed 0.5 cm warty lesion on the right foot, proximal to the great toe. There was satellite lesion 1 cm away from the warty growth. The patient did not notice these lesions. Right inguinal lymph nodes were enlarged and measured 4 x 3 cm. One of the lymph nodes was subjected to histopathology, which also revealed metastatic deposits of malignant melanoma. Wide excision of the lesion with grafting and block dissection of the draining lymph nodes was advised. Patient refused consent for surgical intervention. He succumbed to the disease 3 months later. Discussion Malignant melanoma has a propensity to metastasize widely. Postmortem examination has demonstrated that up to 60% involve small intestine.[1] The current rate of developing melanoma in United States is 1 in 87 and occult metastatic disease is diagnosed in 15% of patients.[2] Small bowel is the most common site of involvement, especially distal jejunum and ileum.[5] Stomach is involved in 27%, large bowel in 22% and esophagus in 5% of cases.[6] Metastatic lesions can be solitary or multiple.[7] Ollila et al reported in their series that resection of involved small bowel had a good prognosis.[8] Medium survival in their group was 48 months. Complete resection of all metastasis in the small bowel yielded a 5-year survival of 38%. Without surgical resection, the prognosis in these patients is poor.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06063f2.jpg] [is06063f1.jpg] |
| |||||||||

{kind=link}
{kind=link}