 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
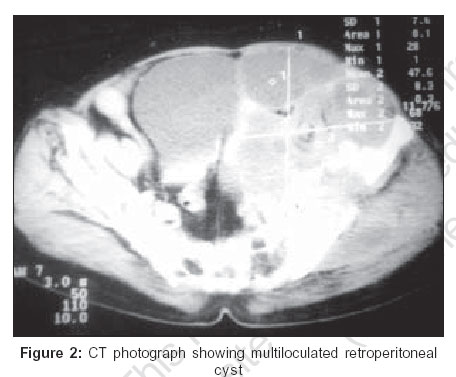
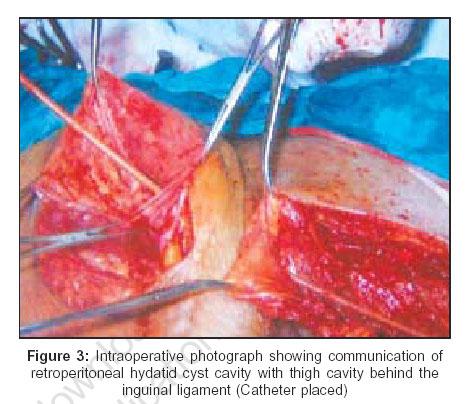
Indian Journal of Surgery, Vol. 68, No. 5, September-October, 2006, pp. 265-266 Case Report Migration of retroperitoneal hydatid cyst into the thigh: A rare presentation Dinesh K. Sarda, Swati J. Lohiya, Varsha G. Jawandiya*, Ashok T. Kamble** Departments of Surgery, *Radiology and **General Surgery, Indira Gandhi Medical College, Nagpur, Maharashatra, India Code Number: is06074 Abstract Primary retroperitoneal hydatid cyst is a rare entity. Migration of retroperitoneal hydatid into the thigh is extremely rare. Retroperitoneal hydatid cyst may migrate along the fascial planes making their presence in the thigh. We report a case of primary retroperitoneal hydatid cyst which presented with asymptomatic thigh swelling with incidentally detected abdominal lump. On exploration both swellings were found to be communicating.Keywords: Cyst, hydatid, unusual location - echinococcosis Introduction Hydatid cyst is a zoonotic disease seen mainly in the tropical countries like India. Retroperitoneum as involvement of hydatid cyst is unusual. Case report A 60-year-old female presented with complaint of asymptomatic swelling on the left thigh since three months. On examination there was a huge soft tissue swelling (15 x 20 cm) on the medial aspect of the left thigh. Per abdominally retroperitoneal lump was found in the left flank [Figure - 1]. (Patient was unaware of abdominal lump.) Abdominal ultrasound and CT scan showed a single multiloculated retroperitoneal cyst [Figure - 2]. A clinical diagnosis of retroperitoneal hydatid cyst with concomitant soft tissue swelling was kept. Indirect hemagglutination assay (IHA) for hydatid was positive. To avoid intraoperative contamination of hydatid, surgery started with thigh swelling first. After incising deep fascia instead of soft tissue swelling, semisolid jelly-like material with daughter cysts was found. All daughter cysts were removed. However, the cavity was extending upward behind the inguinal ligament. Abdomen was opened by left oblique infraumbillical incision. Abdominal exploration showed large retroperitoneal multiloculated hydatid with multiple daughter cysts. Surprisingly, the cavity of the abdominal cyst was communicating with the cavity of the cyst in the thigh behind the inguinal ligament [Figure - 3]. Both cavities were washed with scolicidal agent (1% cetrimide). Postoperative period was uneventful. Patient was discharged on the 14th day. Patient received albendazole for three months. Serial serological investigations showed gradual fall in hydatid antibody titer. There was no recurrence in two-year follow-up.Discussion Echinococcosis is caused by larval tapeworm of genus Echinococcus granulosus (most common), E. multilocularis E. oligarthrus. Hydatid disease is endemic in central India. It presents major health problem in sheep and cattle-rearing countries. The primary host is dog, humans are the intermediate host. Eggs released in dog′s feces when ingested by man, releases oncospheres, which penetrate intestinal mucosa and enter the blood stream to develop into hydatid cysts in multiple organs. Occurrence of hydatid cysts in the liver (60%), in lungs (30%), kidney (2.5%), heart (2.5%) and < 2% in bone, spleen, muscle and brain have been reported.[1] Rare sites are orbit, urinary bladder, chest wall, subcutaneous tissue, parotid, thyroid. Hydatid disease involving retroperitoneum is rare. Primary retroperitoneal hydatid consists of cyst developing in fatty tissue in the space behind the posterior parietal peritoneum without any parasitic foci in other organs.[2] Hydatid in retroperitoneal space can follow and migrate along planes with least resistance. Like psoas abscess, it can migrate along retroperitoneal planes to make its first presentation in the groin and thigh as happened in this case. Unusually, primary retroperitoneal hydatid can present as an adrenal mass.[3] Very few reports of migration of hydatid cyst have been reported in the literature. Reports are made where thigh hydatid are often confused with soft tissue swelling. Hence rare presentation of this disease should be considered while assessing soft tissue swelling, particularly in disease-endemic areas.[4] Echinococcosis can be diagnosed by radiological means or serology, both of which however are not definitive. IHA gives only 50-70% sensitivity, with high specificity. Demonstrating parasitic elements i.e., brood capsule, scolices and hooklets in specimens, makes definitive diagnosis. Recent radiological investigations are fairly accurate in establishing diagnosis. Aspiration is avoided when there is suspicion of hydatid disease for fear of anaphylactic shock. In an endemic region of hydatid disease a diagnosis of hydatid cyst of the retroperitoneum must be entertained on coming across a multiseptated cystic retroperitoneal mass. Treatment is surgery. With increasing experience in laparoscopy and retroperitoneoscopy, advantage of minimal access can be offered in cases of retroperitoneal hydatid cyst.[5] Azoles are useful for intraoperative ruptured cyst and to reduce the risk of recurrence.[3]References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06074f2.jpg] [is06074f1.jpg] [is06074f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}