 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 68, No. 5, September-October, 2006, pp. 269-271 Case Report Solid-cystic papillary tumor of the pancreas: A missed diagnosis Melroy D’Souza, Philip Abraham*, Sudeep R. Shah Divisions of Gastrointestinal Surgery and *Gastroenterology, P.D. Hinduja National Hospital and Medical Research Centre,
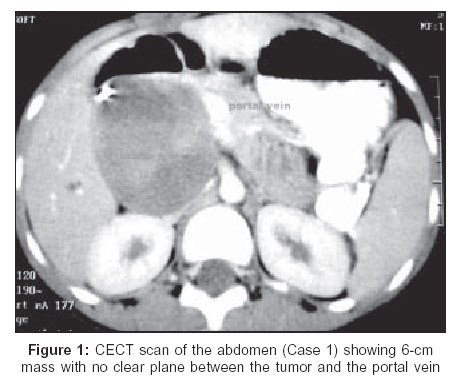
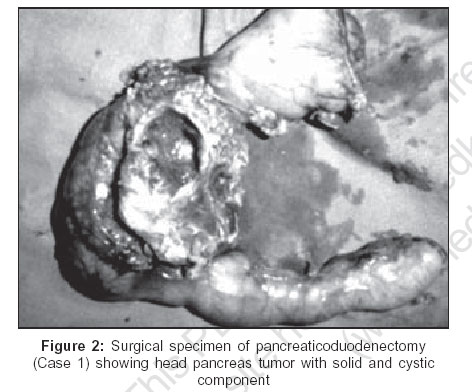
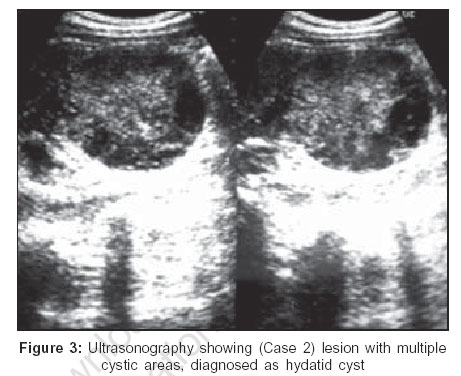
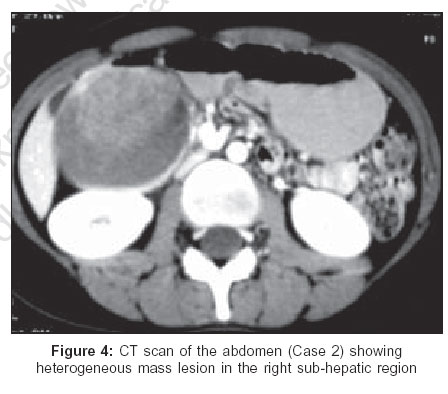
Mahim, Mumbai, India Code Number: is06076 Abstract Solid-cystic papillary tumor (SCPT) of the pancreas is a rare neoplasm mainly affecting young women. The clinical presentation is usually nonspecific. A common problem encountered is misdiagnosis of the tumor on imaging. We report two patients with SCPT of the pancreas diagnosed incorrectly on preoperative imaging. Any cystic lesion of the pancreas with solid elements on radiology should raise the suspicion of this diagnosis. Considered to be a tumor of low malignant potential, surgical resection is associated with excellent prognosis. Surgery may be conservative in localized tumors and aggressive if nonlocalized.Keywords: Pancreas, pancreatic tumor, solid-cystic papillary tumor of the pancreas Introduction Solid-cystic papillary tumor [SCPT] of the pancreas is a neoplasm of low malignant potential found primarily in young women. Though rare, the incidence of this tumor has been increasing in recent years. Surgical resection is associated with an excellent prognosis. However, the main preoperative problem encountered is misdiagnosis of the tumor on imaging. Our report of two patients with SCPT of the pancreas highlights this concern.Case Reports Case 1 An 11-year-old girl presented with history of upper abdominal pain for which she was investigated elsewhere one year previously and was found to have a cystic lesion of the pancreas on imaging. A diagnosis of pancreatic pseudocyst was made and cystogastrostomy was planned. At surgery the surgeon discovered that the lesion had solid components and hence abandoned the procedure. On follow-up the mass increased in size on imaging and the patient developed obstructive jaundice. She underwent an ERCP with stenting of the common bile duct to relieve the jaundice. The patient was then referred to us for further management. CT scan [Figure - 1] showed a mass in the head of the pancreas with no clear plane between the tumor and the portal vein. At surgery a 6 cm-diameter mass was found in the pancreatic head involving a segment of the portal vein. There were no metastases to the liver, peritoneum or lymph nodes. She underwent a pylorus-preserving pancreaticoduodenectomy with portal vein reconstruction. The histological diagnosis was SCPT of the pancreas [Figure - 2]. Her postoperative recovery was uneventful and the patient is alive and disease-free 31 months later. Case 2 A 19-year-old girl presented with history of upper abdominal pain of one month duration. Physical examination revealed a large lump in the right hypochondrium. All laboratory parameters were normal. Ultrasonography [Figure - 3] revealed an 8 x 6 cm lesion with multiple cystic areas within abutting the liver. This was thought to be a hydatid cyst. CT scan [Figure - 4] showed a well-defined lesion in the right sub-hepatic region abutting the liver edge, head of pancreas, duodenum and pylorus. The differential diagnosis included enteric duplication cyst and gastrointestinal stromal tumor. Intraoperatively an 8 cm- diameter spherical mass arising from the head of the pancreas and firmly adherent to the duodenum, bile duct and pancreatic duct was found. There were no metastases to the liver, peritoneum or lymph nodes. A pylorus-preserving pancreaticoduodenecotmy was performed. Histology showed SCPT of the pancreas. Her postoperative recovery was uneventful and the patient is well and disease-free three months later. Discussion Described for the first time by Frantz in 1959,[1] SCPT of the pancreas is a rare tumor representing about 2% of all pancreatic tumors and 9.3% of cystic pancreatic neoplasms.[2] A review of the literature reveals an increasing incidence of these tumors, although it may be that it is increasingly being diagnosed. Papavramidis and Papavramidis in 2005 reviewed 718 cases of the tumor.[3] The clinical features of SCPT of the pancreas are relatively nonspecific, ranging from vague abdominal discomfort to pain and rarely jaundice. Physical examination may reveal a palpable abdominal mass. Nearly 90% of the patients are female with a mean age of 25 years.[4] It is unusual that our first case was an 11-year-old girl who presented with jaundice which too is quite uncommon. Preoperative recognition is essential since surgical resection leads to an excellent prognosis as the tumor has a relatively indolent course. Herein, however lies the problem. Laboratory investigations provide little information and therefore imaging is crucial. Ultrasonographic findings are uncharacteristic and highly variable. Two common patterns are a well-defined hyperechoic mass with or without echo-poor areas.[5] In addition the lesion is sharply demarcated and shows no internal septation.[6] Endoscopic ultrasonography may provide a diagnosis in tumors < 2 cm. CT scan in combination with fine needle aspiration cytology can provide valuable information. The appearance on CT scan is variable and the tumor is sharply circumscribed, well encapsulated and hypodense.[7] A thick capsule is usually seen with the internal architecture comprising mixed solid and cystic components. Calcification may be seen.[8] MRI shows a similar picture. The imaging differential diagnoses include exocrine and endocrine tumors, congenital pancreatic cysts, hydatid cysts, mucinous cystic neoplasms, pancreatoblastoma, cystic lymphangioma and pancreatic pseudocyst. Differentiation of SCPT from these is vital. Solid elements within a cystic lesion on imaging should always raise the suspicion of a SCPT of the pancreas. Given the low malignant potential of this tumor, conservative resections such as enucleation, lumpectomy and partial resection have been attempted with favorable outcome and may be considered, especially in pediatric patients.[9],[10] Complete resection is the mainstay of treatment and the operation chosen depends on the location of the tumor and its spread. Diagnosis can be confirmed intraoperatively by frozen section. The standard surgical approach involves complete removal of the tumor with involved pancreas, all associated lymph nodes and any adjacent involved organs. Local invasion, limited metastases, recurrence and even portal vein invasion are not considered contraindications to resection[3],[4],[10] and should be appropriately dealt with. Chemotherapy and radiotherapy have no clearly defined role in treatment. Prognosis of SCPT of the pancreas is good with a five-year survival rate of 95% and even patients with metastatic disease may have long-term survival.[3] SCPT of the pancreas is a neoplasm of low malignant potential. It principally affects young women. A cystic lesion of the pancreas having solid elements should always raise the suspicion of a SCPT. Complete surgical removal is associated with an excellent prognosis. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06076f4.jpg] [is06076f3.jpg] [is06076f1.jpg] [is06076f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}