 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 68, No. 5, September-October, 2006, pp. 272-274 Case Report A rare case of primary pancreatic tuberculosis mimicking neoplasm Melroy D’Souza, Philip Abraham*, Sudeep R. Shah Divisions of Gastrointestinal Surgery and *Gastroenterology, P.D. Hinduja National Hospital and Medical Research Centre,
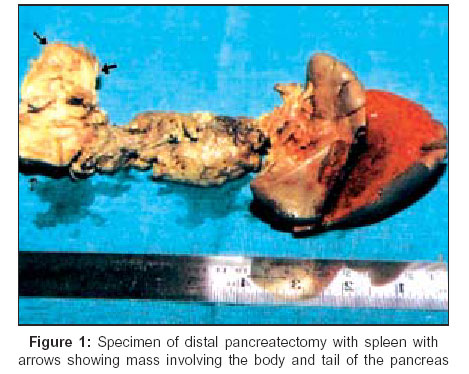
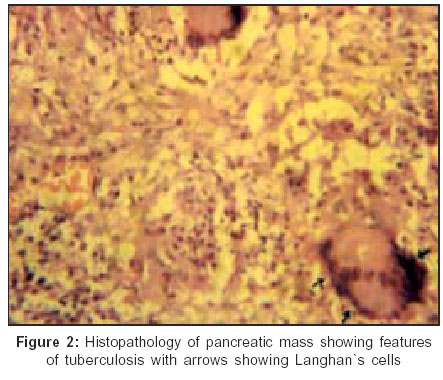
Mahim, Mumbai, India Code Number: is06077 Abstract We report a rare case of a 28-year-old man who presented with vague intermittent upper abdomen pain for six months and a lump of 6 x 4 cm size in the epigastric region for three months. His human immunodeficiency virus serology was negative and a Mantoux test was nonreactive. CECT of the abdomen showed a soft tissue mass involving the body and tail of the pancreas, with mild dilatation of the pancreatic duct suggestive of neoplasm. Results of CT-guided fine needle aspiration cytology were inconclusive. Exploratory laparotomy revealed a firm pancreatic mass in the body and tail of the pancreas, approximately 6 x 4.2 x 3.2 cm in size Histopathology revealed caseating granulomas and presence of giant langhans cells suggestive of tuberculosis. Although primary pancreatic tuberculosis is rare it should be considered among the differential diagnoses, especially in young patients who present with a mass in the pancreas, particularly in developing countries and immunocompromised patients worldwide.Keywords: Abdominal tuberculosis, pancreatic neoplasm, primary pancreatic tuberculosis Introduction Primary pancreatic tuberculosis is a very rare occurrence in the setting of extra-pulmonary tuberculosis. It usually occurs as a complication of miliary tuberculosis in immunodeficient individuals, particularly with HIV infections, but isolated visceral involvement in an immunocompetent patient is extremely rare.[1] Diagnosis of primary tuberculosis of the pancreas is often missed, because of very low incidence and as most of the time it mimics pancreatic neoplasm.[2] We report a case of a young patient who underwent exploratory laparotomy for a pancreatic mass and was later found to have pancreatic tuberculosis on histopathology. This report emphasizes the importance of high clinical suspicion and preoperative diagnostic workup for primary isolated tuberculosis of the pancreas in young patients even if they are immunocompetent. Case report A 28-year-old male presented with pain in the epigastric region for six months associated with an epigastric lump that had been gradually increasing in size for three months. He also had a history of low-grade intermittent fever since two months. He had lost five kilograms of weight over the preceding year. Abdominal examination showed a well-defined spherical, nonpulsatile, nontender lump of size 6 x 4 cm with smooth surface in the epigastric region. Laboratory investigations were normal except ESR that was 55 mm. Chest and abdominal radiographs were normal on many occasions. HIV serology was negative and a mantoux test was nonreactive. Abdominal ultrasonography revealed a hypoechoic lesion in the body and tail of the pancreas of size 5.8 x 3.8 cm, suggestive of neoplasm. Contrast enhanced CT scan of abdomen showed a well-defined, soft tissue mass involving the body and tail of the pancreas, measuring approximately 6 x 4.2 x 3.2 cm in size with obliteration of fat planes in this region with mild dilatation of the distalmost part of the pancreatic duct suggestive of pancreatic neoplasm. There was no evidence of lymphadenopathy on CT scan. Results of CT-guided fine needle aspiration cytology (FNAC) were inconclusive. Repeat FNAC showed hemorrhagic aspirate. Exploratory laparotomy revealed a firm pancreatic mass in the body and tail of the pancreas approximately 6 x 4.2 x 3.2 cm in size [Figure - 1]. There was no evidence of any gross pathological involvement of the gastrointestinal tract, the mesentery, its nodes, omentum, the peritoneum, and other solid organs such as liver, gall bladder and spleen. Peroperative frozen section at laparotomy was not done. Distal pancreatectomy with splenectomy was done thinking neoplastic pathology of the body and tail of the pancreas. Histopathological examination revealed caseating granulomas and presence of giant langhans cells suggestive of tuberculosis [Figure - 2]. Following the histological diagnosis of pancreatic tuberculosis, the patient was successfully treated with antituberculous therapy. Regular three-monthly follow-up of the patient was done for one year and the patient was doing well. Discussion Abdominal tuberculosis is rare in western countries but there has been resurgence of this disease due to the human immunodeficiency virus infection and other immunodeficient states in developed countries. Tuberculosis is still a major public health problem in the economically underprivileged countries. Tuberculosis, in its extra-pulmonary form, though emerging as a clinical problem, rarely affects the pancreas. It usually occurs as a complication of miliary tuberculosis in immunodeficient individuals. In 1944, Auerbach reported that the pancreas was affected in 4.7% of cases of miliary tuberculosis[3] although the low incidence may have been due to under-diagnosis. Pancreas is biologically protected from being infected by Mycobacterium tuberculosis probably because of the presence of pancreatic enzymes that interfere with the seeding of Mycobacterium tuberculosis.[4] The pathogenesis of pancreatic tuberculosis is not very clear. The pancreas can be involved in three ways a) hematogenous dissemination b) by direct spread from contiguous caseating lymph nodes[5] c) reactivation of dormant bacilli in an old tubercular lesion in cases of immunosuppression. Pancreatic tuberculosis presents with symptoms like pancreatic pain, obstructive jaundice, iron deficiency anemia, pancreatic abscess, massive gastrointestinal bleeding, acute/chronic pancreatitis, secondary diabetes, splenic vein thrombosis and a pancreatic mass mimicking pancreatic malignancy.[4] The Mantoux test is usually strongly positive but may be equivocal. Plain radiograph of chest may show some evidence of tuberculosis but may be normal. The diagnosis can be established by ultrasonography or CT-guided FNAC.[1] But the diagnostic accuracy of FNAC has not been proven and exploratory laparotomy[6] may be required in technically difficult cases due to risk of injury to the vessels in the vicinity of the mass.[4],[6] Many patients improve dramatically with antitubercular treatment,[2],[4] if diagnosis is made preoperatively. Our patient fulfils all the criteria for the diagnosis of primary pancreatic tuberculosis. He had no history of tuberculosis, the disease was localized, his chest radiograph was normal, he had no other detectable foci of tuberculosis with no peripancreatic and other lymphadenopathy and also, the patient was not immunocompromized and a positive cytological diagnosis was made. However, preoperative diagnosis in our case could not be made because FNAC was inconclusive and chest radiograph was normal. It is evident from the literature that many a times diagnosis of pancreatic tuberculosis is not suspected prior to laparotomy.[4],[7] We conclude that especially in young patients who present with a mass in the pancreas, pancreatic tuberculosis should be considered among the differential diagnoses, particularly in developing countries. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06077f2.jpg] [is06077f1.jpg] |
| |||||||||

{kind=link}
{kind=link}