 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
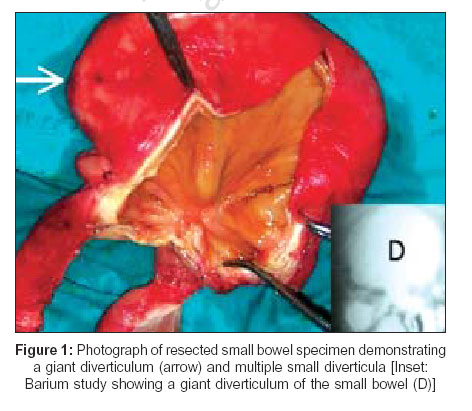
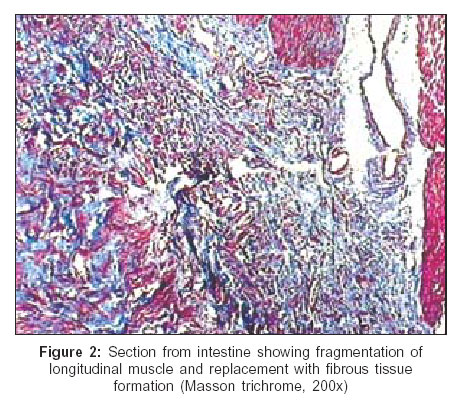
Indian Journal of Surgery, Vol. 68, No. 5, September-October, 2006, pp. 275-277 Case Report Small intestinal diverticulosis presenting as anasarca K. Harish, R. Harikumar, V. Thomas, M. Feroze*, P. Rajan** Departments of Gastroenterology, *Pathology and **Surgery, Calicut Medical College, Calicut - 673 008, Kerala, India Code Number: is06078 Abstract Diverticulosis of the small bowel is uncommon. Most cases are asymptomatic and are often discovered incidentally. Small intestinal diverticulosis presenting as anasarca and leading to life-threatening complications is very unusual. We report a 20-year-old male who presented with chronic small bowel diarrhea, ascites and generalized edema. Barium studies and CT abdomen showed evidence of a large diverticulum arising from the small bowel. He developed intestinal obstruction and perforation requiring exploratory laparotomy which showed one large and several small diverticula in the ileum. Resection and end-to-end anastomosis was done, but in the postoperative period he succumbed to unrelenting septicemia. Histopathology of the excised small intestine was consistent with visceral myopathy.Keywords: Anasarca, ascites, intestinal obstruction, malnutrition, perforation, small-bowel diverticulosis Introduction Small bowel diverticulosis (SBD) is a rare entity and is generally considered to be an innocuous condition. Most cases are usually asymptomatic. We hereby report a case of ileal diverticulosis presenting with severe malnutrition and anasarca leading to perforation and peritonitis requiring emergency surgery.Case report A 20-year-old male presented with history of progressive abdominal distension and generalized edema since one month. He had history of intermittent upper abdominal pain and large volume diarrhea since one year. Personal and family history was noncontributory. On examination, he was emaciated with BMI of 17; he had pallor and generalized edema. Clinical examination of the cardiovascular, respiratory and nervous system was unremarkable. Investigations hemoglobin 8.7 g/dl (13.5-16.5 g/dl) with mean corpuscular volume 124 mm3 (78-100 mm3), total white cell count 7800/mm3 (4000-10000/mm3), platelet count 170,000/mm3 (150000-350000/mm3) and peripheral smear suggestive of megaloblastic anemia. Other biochemical tests included serum albumin 2.2 g/dl (3.2-5.5 g/dl), serum calcium 7.2 mg/dl (9-11 mg/dl), serum cholesterol 108 mg/dl, vitamin B12 levels 176 pg/ml (200-800 pg/ml) and serum folate 7.5 ng/ml (3.1-17.5 ng/ml). Repeated stool examinations and a thorough search for parasites and other diarrheal pathogens were negative. The stool was also guaiac negative. Doppler ultrasonography showed ascites, fatty liver and a patent portal vein. Serologic studies for antinuclear antibodies, anti-double stranded DNA, rheumatoid factor and Scl-70 were negative. Serum-ascetic fluid albumin gradient was low (0.6 g/dl). Twenty-four hour fecal fat measurement revealed steatorrhea of 18.6 g fat/24 h (normal range < 7 g/24 h). D-Xylose absorption test (25 g) showed excretion of 2g in urine within 5 h of ingestion (normal 6 ± 1.5 g). Upper endoscopy and colonoscopy up to terminal ileum was normal. Histology of the duodenal and terminal ileal mucosa revealed no abnormal findings. Barium meal follow-through showed a focal dilatation of the proximal ileum measuring 10 cm in length and 8 cm in diameter with normal ileal loops proximally and distally and was interpreted as a ′giant′ ileal diverticulum [Figure - 1]. The rest of the small bowel showed normal mucosal pattern and diameter with no focal dilatations or outpouchings. There was no mechanical obstruction and the colon appeared normal. A helical CT abdomen with oral contrast also showed the dilated loop of the small bowel communicating with the ileum, suggestive of an ileal diverticulum. The patient was treated with tetracycline (500 mg QID), metronidazole (250 mg BID) and high-protein, low-residue diet supplemented with parenteral nutrition. On the 18th hospital day, he developed severe colicky periumbilical pain with vomiting and high grade fever. The abdominal X-ray film revealed multiple air-fluid levels and dilatation of the small bowel; there was no free peritoneal air. Ascitic fluid was turbid and revealed total count of 10,200 with 80% neutrophils, total protein 3.5 g/dl, LDH 450 U/L and glucose was undetectable. He was started with broad-spectrum antibiotics and received nothing by mouth. Our diagnosis was diverticulitis with suspicion of covert perforation. An exploratory laparotomy was done; at surgery ascitic fluid was found in the peritoneal cavity with small bowel appearing dilated and matted together with multiple small diverticula in the ileum with a giant diverticulum which contained a small irregular perforation covered by soft grayish material [Figure - 1]. The distal ileum, jejunum and the entire colon appeared normal. All grossly involved small bowel was resected and end-to-end anastomosis was done. Histopathologic examination of the excised small intestine, both from diverticular wall and in the areas between the diverticula revealed degeneration, thinning and fragmentation of the smooth muscle, especially the longitudinal muscle layer. The myenteric plexus was normal. Masson′s trichrome stain showed muscle fragmentation and replacement with fibrous tissue formation [Figure - 2]. A diagnosis of visceral myopathy with ileal diverticulosis was made. On the 12th postoperative day, while on cefotaxime (2 g intravenous q8h) and metronidazole (500 mg intravenous q8h), he developed fever, tachypnoea, tachycardia and generalized bleeding tendency. Laboratory investigations revealed total white cell count of 16,300 (90% neutrophils), platelet count of 62,000 per mm3, PT (INR) of 3.2 and peripheral smear showing neutrophilia with toxic granules. Serum fibrinogen was low (100 mg/dl) and fibrin degradation product was positive though blood culture revealed no growth. There was no anastomotic leakage or any abscess localized in the abdomen. Patient was treated with meropenam 1g intravenous q6h, clindamycin 600mg intravenous q8h, three units of platelet transfusions and ten units of fresh frozen plasma. Later he developed hypotension and respiratory failure requiring ionotropic and ventilatory support. Despite these measures his condition progressively deteriorated and he succumbed to unrelenting septicemia on the 28th postoperative day. Discussion Diverticulosis of the small bowel is uncommon, having a reported incidence of 1 to 2% in the general population.[1] Eighty per cent of jejunoileal diverticula are localized to the jejunum, 15% to the ileum and 5% to both. Most cases of small bowel diverticula occur during the 6th and 7th decades and are very rarely described in children.[2] They are frequently associated with disorders of intestinal motility, such as progressive systemic sclerosis, visceral neuropathies and myopathies.[3] It is usually an incidental finding detected during barium studies, majority of patients being asymptomatic. Serious complications, though rare, occur in about 10% of them and include bleeding, malabsorption, infection, diverticulitis with or without perforation, intestinal obstruction and pseudo-obstruction.[4] Malabsorption due to bacterial overgrowth occurs in about 3-12% and may lead to megaloblastic anemia, hypoproteinemia and steatorrhea. The gold standard for the diagnosis of bacterial overgrowth is quantitative culture of small bowel aspirate. Alternatives include xylose and hydrogen breath tests. Mechanical obstruction is another frequent complication and may be a consequence of volvulus, stricture or adhesions from prior diverticulitis, neoplasia, intussuception or enterolith formation.[5] Pseudo-obstruction has also been reported in 10-25% of cases.[6] An underlying bowel visceral myopathy, neuropathy or clinically inapparent progressive systemic sclerosis is usually the culprit.[3] Malabsorption due to bacterial overgrowth caused by stasis within the diverticula is treated with broad-spectrum antibiotics.[7] However surgical or laparoscopy-assisted resection of the involved segment is indicated in patients with diverticulitis, bowel obstruction, perforation or bleeding. In our case the diagnosis of bacterial overgrowth was presumptive based on evidence of malabsorption with cobalamine deficiency in a background dysmotility with diverticulum, as small bowel aspirate and breath tests were not done. Moreover, no other causes were revealed by the diagnostic tests including repeated stool tests, upper and lower endoscopy with biopsies and radiographic imaging. The case described is one of an unusual disease with an uncommon presentation occurring at a very young age, causing life-threatening complications. The rarity of symptomatic diverticula often makes small bowel diverticulosis an overlooked diagnosis. A high index of suspicion, early diagnosis and prompt intervention can have a marked impact on outcome for this often obscure disease. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06078f2.jpg] [is06078f1.jpg] |
| |||||||||

{kind=link}
{kind=link}