 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
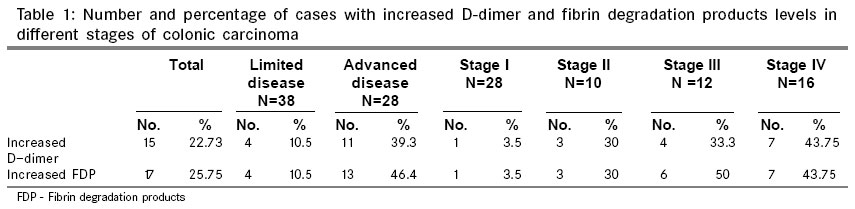
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 306-309 Original Article Do plasma D-dimer levels correlate with disease stage in colonic carcinoma? Subramanian Sitalakshmi, Rameshkumar Karuna, Damodar Prema Department of Clinical Pathology, St.. John's Medical College Hospital, Bangalore - 560 034 Code Number: is06089 Abstract Background: Hemostasis is deeply involved in tumour growth, angiogenesis and metastasis. Patients with cancer may harbor many alterations of hemostasis and these are multifaceted. The hemostatic changes have been correlated with bulk of tumour and overall patient survival. Keywords: Colonic carcinoma, D-dimer, stage Introduction The coagulation dysfunctions of different nature and magnitude, ranging from subtle laboratory abnormalities to overt thromboembolism and DIC are routinely found in cancer patients.[1] Tumour tissue is the source of both procoagulant and fibrinolytic activities. Fibin(ogen) is important in tumour stroma formation. Fibrin and fibrin degradation products (FDP) have chemotactic, immuno modulatory as well as angiogenic properties and thus play an important role in tumour progression. Fibrinogen is an important determinant of the metastatic potential of circulating tumour cells.[2].[3] Fibrin turnover in the tumour extracellular matrix is essential for tumour angiogenesis and growth Crosslinked fibrin in the extracellular matrix serves as a stable framework for endothelial cell migration during angiogenesis and tumour cell migration during invasion. D-dimer is a stable end product of fibrin degradation and its levels are elevated by enhanced fibrin formation and fibrinolysis. It is produced when both intravascular and extravascular cross linked fibrin is degraded by plasmin. Plasma D-dimer level is reportedly elevated in patients with solid tumours including colorectal cancer, lung cancer, ovarian malignancies, prostatic cancer and breast cancer. Among patients with colorectal cancer, breast cancer, ovarian malignancies, higher plasma D-dimer levels have been shown to correlate with more advanced tumours. Plasma D-dimer levels have been shown to be directly correlated with tumour markers like CEA.[4] This study was aimed at assessing whether plasma D-dimer measurement correlates with stage of the disease in patients with colonic adenocarcinoma. Materials and methods This was a prospective study of biopsy proven adenocarcinoma colon conducted over a period of two years from January 2003 to December 2005. Sixty-six consecutive new cases of adenocarcinoma colon were included. Patient information including age, sex, presenting complaints, relevant history was obtained to rule out any bleeding disorder, liver disease, H/O drug intake, physical examination, provisional clinical diagnosis, histopathological / cytological diagnosis and details of treatment. Information regarding tumour site, histological diagnosis, tumour differentiation and postsurgical staging was recorded. Details of other investigations like biochemical-liver function tests, tumour marker levels, baseline hematological and coagulation parameters, radiological, ultrasonological, computed tomography (CT) scan, magnetic resonance imaging and bone scan were noted in relevant cases. The presence of metastatic disease was determined by one or more of the following: physical examination, chest X-ray, ultrasonological examination of abdomen and pelvis, CT scan, bone scan, fine needle aspiration cytology or other tissue / cytological diagnosis. All cases (both male and female) with biopsy / cytology proven diagnosis of adenocarcinoma colon in the age group 21-90 years were included at the time of diagnosis. Patients on anticoagulant therapy, subjects taking oral contraceptives, those with liver disease, inherited bleeding disorder and pregnant women were excluded. The baseline coagulation tests like platelet count, prothrombin time and activated partial thromboplastin time were performed. The plasma D-dimer and FDP levels were measured by latex agglutination immunoassay test in all the cases at the time of diagnosis. The D-dimer test is a semi-quantitative determination of crosslinked fibrin derivatives (containing the D-dimer domain) in human plasma by using fibronosticon kit (bioMerieux). The kit uses latex particles, which are coated with anti-D-dimer murine monoclonal antibodies. These latex particles form macroscopic aggregates only in the presence of fibrin derivative containing the D-dimer domain. The kit used for FDP assay (Diagnostica Stago) is latex immunoassay. The latex particles are coated with a monoclonal antibody which reacts with fibrin and fibrinogen degradation products macroscopic agglutination is looked for and the dilution at which a negative result is obtained is noted as compared to the response of the positive and negative controls. The results were read as follows: Undiluted negative: < 500 ng/ml for D-dimer and The results of the D-dimer and FDP test were grouped into two - < 500 ng/ml (normal) and> 500 ng/ml (high) for D-dimer and < 5 mg/ml (normal) and > 5mg/ml (high) The cases were grouped into different stages based on the TNM classification. Statistical methods Chi-square distribution test was applied to compare the results of the D-dimer and FDP tests across the four stages using incidence data depending on the number of cases in each range group (normal and high range groups). Mann Whitney U test, which is a nonparametric tests was applied between limited disease and advanced disease to test the variation. The study was approved by the institutional ethical review board and informed consent was obtained from all cases. Results The study included 66 cases of biopsy proven adenocarcinoma colon - (44 males and 22 females). Age ranged from 28 to 82 years. There were 28 cases in stage I, 10 in stage II, 12 in stage III and 16cases in stage IV. Stage I and II were considered as limited disease (38 cases) and stage III and IV as advanced /extensive disease (28 cases). The test results were classified into two groups-normal and high. The number and percentage of cases showing an increased D-dimer and FDP levels among the total 66 cases, among the limited and advanced disease and among all cases in stage I, II, III and IV are shown in [Table - 1]. It was observed that the percentage of cases with increased D-dimer and FDP values were higher in the advanced disease when compared to limited disease. It was also noted that the percentage of cases with increased D-dimer and FDP values increased with the stage of the disease. Chi square test showed statistically significant difference when the results of D-dimer ( P 0.05 and degree of freedom is 2) and FDP ( P 0.01 and degree of freedom is 2) were compared across the four stages. When the results were compared between limited and advanced disease by Chi square and Mann Whitney U test, they were found to be statistically significant . ( P 0.05) [Table - 2]. Discussion The laboratory findings in patients with malignancies reflect, in general, activation of the coagulation system and compensatory fibrinolysis. These interacting processes proceed at variable rates depending upon the type of tumour, extent of tumour burden, treatment and complications like sepsis.[5],[10] Gang assessed the clinical significance of D-dimer levels and the relationship between plasma D-dimer and clinicopathologic parameters in operable colorectal cancer patients. They measured plasma levels of D-dimer pre and postoperatively in 35 patients with colorectal cancer and 30 healthy controls by enzyme-linked immunosorbent assay. They observed that the mean preoperative plasma. D-dimer levels in the patients with colorectal cancer were significantly higher than those of controls. It was also observed that the preoperative levels of D-dimer were significantly correlated with lymph node metastasis and Dukes stage but had no association with tumour location and degree of differentiation. A stepwise increase in the mean D-dimer levels was found with increase of tumour stage.[6] The relationship between preoperative plasma D-dimer level and both pathological findings and TNM classification and the prognostic significance of preoperative plasma D-dimer level was examined by Oya et al in 93 patients who underwent curative resection of colorectal cancer. There were seven cases in stage 0, 10 cases in stage I, 30 in stage II and 36 in stage III. They found that the plasma D-dimer levels were significantly higher in patients with moderately differentiated adenocarcinoma, larger tumours, deep-wall penetration and advanced TNM stages The factors that were found to be associated with shorter postoperative survival were histological types other than well-differentiated adenocarcinoma, advanced tumour stage, the presence of lymphatic and venous invasion, high preoperative D-dimer and serum CEA levels. Results of analysis with a multivariate proportional hazard model suggested that preoperative plasma D-dimer level was the third strongest prognostic factor, exceeded in importance only by lymph node status and preoperative CEA level.[7] Our study showed increased D-dimer levels in 39.3% of the cases in advanced disease as compared to 10.3% of the cases in the limited disease as also seen in the study of Edwards et al .[8] Significant correlation between baseline D-dimer values and CEA levels, tumour burden and the number of metastatic sites was demonstrated by Blackwell et al in 98 patients with metastatic colorectal carcinoma. In addition, patients with liver metastases and patients with lung metastases had higher D-dimer values. They also showed that elevation in D-dimer values exhibited a stronger correlation with disease progression than did CEA levels . The authors conclude that a direct correlation exists between D-dimer levels and overall survival in colorectal cancer and also the correlation of serial D-dimer values with disease progression.[3] This study supports the fact that the activation of the hemostatic system is an integral part of colonic carcinoma.[9],[10] The plasma levels of breakdown products of the fibrin like the D-dimer and FDP which are found to correlate with the disease stage may provide useful supplementary information to disease stage.[10] The interpretation of coagulation studies in cancer are confounded by several factors, one of which is the selection of cases. This study has avoided this by choosing cases with only one histological type of cancer involving one site, adenocarcinoma colon. The usefulness of D-dimer in predicting disease progression in colorectal carcinoma remains to be determined by long term follow-up and repeated sampling. Conclusion Myriad of clotting defects in malignancies have been uncovered by sophisticated laboratory tests. Of these, measurement of plasma D-dimer levels using commercially available kits is neither complicated nor time consuming. If it is included in the routine preoperative laboratory examination of patients with colorectal cancer, it can provide supplementary information on tumour stage and prognosis.Acknowledgements Ramweshwardas Birla Smarak Kosh, Mumbai, Karnataka Medical Education Research Trust, Bangalore. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06089t1.jpg] [is06089t2.jpg] |
| |||||||||

{kind=link}
{kind=link}