 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
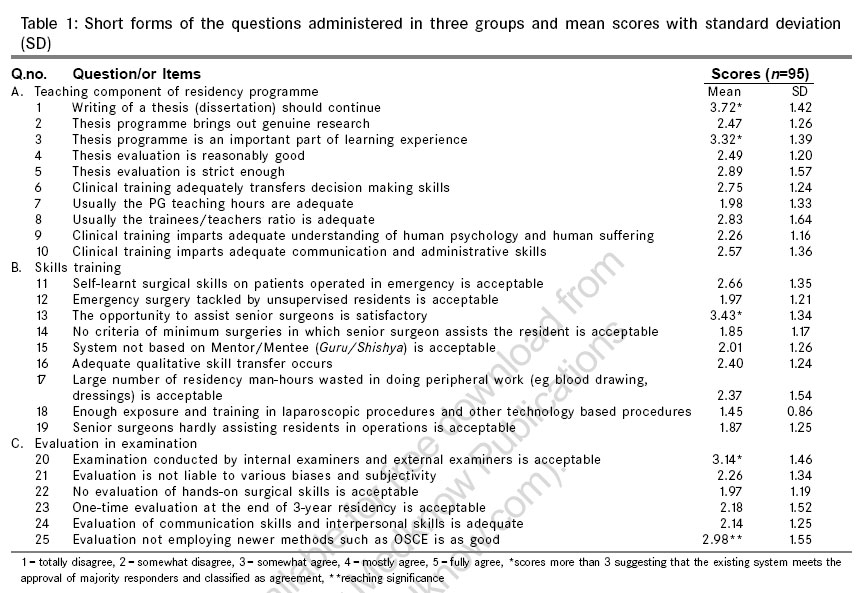
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 310-315 Original Article Surgical residency programme: Training, teaching, and evaluation in general surgery -A peer opinion poll in five medical colleges in northern India Gupta Anubhav, Kumar Surender, Kumar Shailendra, Mishra MC, Kumar Sandeep Department of Surgical Sciences, All India Institute of Medical Sciences, New Delhi Code Number: is06090 Abstract Background: Teaching, training, and evaluation in general surgery has not been peer reviewed in India. An archaic 3 years residency, thesis writing, and evaluation at the end of 3 years leading to award of master's degree (MS) in general surgery has continued since 1950s. Immense growth in knowledge, emergence of new sub-specialties and surgical technologies has mandated a change in the existing surgical residency programme.Aim: To obtain a peer opinion on the existing surgical residency programme. Setting and Design: Cross sectional survey, 70 residents and 25 surgical teachers of five medical institutions, a pilot study in northern India. Materials and Methods: A close ended, interviewer-administered questionnaire based on 5-point Likert scale with 25 items of teaching, training, and evaluation on existing PG surgical residency programme. Results: Majority subjects felt that thesis was an important part of learning experience and it should continue. Opportunity to assist senior surgeons was adequate, but seniors should also assist the resident surgeon under training, a mentor-mentee type training pattern should be evolved, multiple evaluations on content, surgical skills, ethical, and managerial skills should evolve rather than a single examination conducted by internal/external examiners at the place of training after 3 years. A 5-years MCh in general surgery for academically oriented students including exclusive training in minimally invasive procedures, clinical epidemiology, pre-hospital and trauma management, and vascular surgery was suggested by many responders for a limited number of seats in general suregry. Conclusion: Broad-based training during general surgical residency in theoretical knowledge, open and endoscopic surgical skills, research methodology, critical appraisal, ethics and inter-personal skills should be part of revised programme along with multi-point evaluation and thesis writing. Keywords: General surgery, peer review, surgical residency programme Introduction Three years in-house training imparting surgical skills, ability to collect and analyze data and write a dissertation, theory examination on the content and clinical examination to test the abilities to recognize signs and symptoms, and communication skills and manners have been mandated by the Medical Council of India (MCI) for accrediting masters in general surgery all over the country in the year 2001.[1] The above description of surgical training by MCI appears adequate; however, the actual implementation and quality control may not be uniform. Voices have been raised to modify the MS (general surgery) programme from time to time especially because of extensive growth in knowledge base, development of sub-specialties and new technologies. There is no published report in the peer-reviewed Indian surgical journals on the subject of teaching, training, and evaluation in surgery. The field of surgery is an ever-evolving one, and there is a need for a system that is acceptable and dynamic to keep pace with the rapidly changing knowledge base and technology. Last decade has witnessed the emergence of minimally invasive surgery and increasing dependence on its applications. There appears to be a slow departure from the classical description of signs and symptoms of various diseases that used to be the basis of clinical diagnosis. The present day textbooks on clinical surgery are devoid of data on clinical prediction rules made from evolving diagnostic algorithms after calculating sensitivities, specificities, and predictive values of the various signs and symptoms singly or in combination. There is also rapid advancement in the super/or sub-specialty branches of surgery leading a void in the general surgery departments that have the responsibility to train the basic surgeons. An amalgam of the above issues mandates a paradigm shift in the present residency-training programme in India. Besides teaching and training the evaluation system for MS examination also needs to be reviewed. At present there is a single point theory and practical examination at the end of 3 years. The vexed issue of thesis evaluation, objective structured clinical examination (OSCE) and examination away from the place of training needs to be discussed. The present study was conducted in five medical teaching institutions with the objective to document the peer opinion of the postgraduate surgical education in our country. The aim of the study was to evolve a judicious method of surgical education, surgical training, and evaluation. This study should also start a process of thinking and debate on training in general surgery. Materials and methods The study subjects consisted of surgical teachers and residents. A matrix of questions was generated on various aspects of general surgery residency programme. The questions on which opinions varied and on the aspects, which were pertinent to the training programme were included. The questions on which there was a general agreement were eliminated. The mesh of the questions evolved from invoking tea-room focus group discussions in the Department of Surgery at Lucknow. The questionnaire was designed[2] to address important issues pertaining to the general surgery residency programme based on a 5 point Likert scale[3],[4] ranging from total disagreement to total agreement for example 1 = totally disagree, 2 = somewhat disagree, 3 = somewhat agree, 4 = mostly agree, 5 = fully agree. All the questions were framed in such a manner that higher scores would reflect the adequacy of the existing system. Some of the questions were deliberately duplicated to test the internal consistency. The questionnaire was piloted in a group of 10 teachers and 10 residents for face validity, content validity, and reliability. A final instrument is outlined in [Table - 1], which was distributed in three groups of A, B, C representing teaching, training, and evaluation, respectively. Besides the structured questions as shown below, open-ended opinion of the respondents were also noted. The present study was conducted by two interviewers (AG + SK) on 70 postgraduate students including junior/senior residents and 25 teachers in Surgery at King George's Medical University, Lucknow (40 and 10), All India Institute of Medical Sciences, New Delhi (8 and 4), Maulana Azad Medical College, New Delhi (7 and 3), Sarojini Naidu Medical College, Agra (9 and 4) and Moti Lal Nehru Medical College, Allahabad (6 and 4). Thus a pre-designed, pre-tested, and self-administered interview schedule aimed at obtaining peer opinion on training in general surgery was administered. In group 'A' (teaching component), there were 10 questions pertaining to the legitimacy of the thesis programme, genuineness of the research dissertations and evaluation of the thesis, adequacy of PG teaching hours and appropriateness of ratio of PG teacher to the PG students. It also enquired about the decision-making skills, administrative, and communication skills imparted by the present system. Whether the present training adequately dealt with human psychology, human suffering, and palliative care was also enquired upon. In group B, 9 questions directed towards skills transfer during the residency programme were included. This encompassed acceptability of unsupervised emergency surgery performed by residents, wasting precious time in peripheral work (forms filling, blood sample collection and labeling, catheterization, IV lines, references, dressings, report collection, dispute, and arbitrations, etc.) that can be accurately done by paramedical staff. Adequacy of exposure and training in laparoscopic and other technology based procedures, opportunity to assist senior surgeons in elective surgery, creation of a criterion of minimum number of operations in which senior surgeons assist the residents, shift to a Mentor-Mentee ( Guru-Shishya ) based system for skills transfer. Group C included 6 items on the evaluation of the residents during the training programme, conduction of examination at the place of training by internal and external examiners, susceptibility of the evaluation to various biases and subjectivities. We further enquired about the acceptance of one time examination at the end of 3-years training programme. The opinion was taken on acceptability of a more strict evaluation system employing newer methods like OSCE and adequacy of the present system in evaluating communication, interpersonal relationship, and operative skills. Results The opinion of teachers and residents on the teaching component of the existing programme were mostly clearly indicated with no ambiguity. The opinion of the residents and that of teachers were alike, and therefore the results have been combined and shown in [Table - 1]. A score> 3 was obtained in four out of 25 items only indicating that the opinion was meagerly supportive of the present system (depicted by FNx01 in [Table - 1]) and in all other aspects (21 out of 25) the responders favored a change from the existing practices (scores < 3 showing disagreement). The scores were in favor of maintaining thesis writing during MS general surgery. Most respondents believed that thesis was an important part of learning experience; however, they acknowledged that in its present form, the thesis programme failed to bring out genuine research. It was perceived as a burden by some (open-ended study). Majority were of the opinion that thesis evaluation should be more stringent in open-ended evaluation, however, a mean score of 2.89 (item no. 5) indicated the responder were happy the way the thesis are evaluated at present. The scores favored an increase in number of formal PG teachers (defined by MCI as a teacher of associate professor rank with a minimum experience of 5 years) and augmenting the PG teaching hours during the training programme. The present system was thought as being weak in sensitizing residents to human sufferings and imparting knowledge in the field of human psychology. The present system was also found lacking on account of imparting adequate administrative and communication skills to the trainee residents. On the skills transfer the scores favored a Mentor-Mentee system of training. Most were of the opinion that a criterion of minimum number of surgery to be performed under direct supervision of senior surgeon should be laid down and there should be more exposure of laparoscopic and other technology based procedures. The mentor-mentee system of longer duration spent with a single teacher during the 3 years course of residency was favoured. On evaluation of the residents during and after the training programme the scores showed that evaluation of skills should also be done. One time examination at the end of the 3 years course was disfavored. Ironically, the respondents were not in favor of OSCE type examination but suspected subjectivity during evaluation. More stress on communication and inter-personal skills ought to be imparted especially clinical manners, attitude towards patients and humane and holistic approach to the patients and family (item no. 24 and open-ended study). Discussion Surgical education in Independent India started in the 1950s, when the MS surgery programme was of 3 years including one year house surgeon and 2 years of resident surgical officer. This system has not undergone any major change in the last 56 years except for the fact that the 3 years training is now known as junior residency years-one, two, and three. This is followed by an evaluation at the end of 3 years and awarding of a degree of masters in surgery. A senior residency programme has been introduced in some colleges, and this has apparently served well for a highly populous and resource deficient country, like India to create surgical human resource for the masses. A peer opinion poll on close-ended questionnaire administered to surgical teachers and residents was conducted in five important medical colleges of northern India to which the results of this study may be applicable. However, it can also provide guidance to similar programme where certain differences exist. Open ended opinions were also recorded. Unless, serious efforts are made to restructure the MS General Surgery programme, the degree of masters in general surgery may fast be devalued. It was in this context that a peer perception was obtained through interview poll and results have been described above. Of the 25 items, only on four items there was a general agreement that the existing system is acceptable and on the remaining 21 items, the scores were low indicating that majority responders voted in favor of change in the current MS general surgery postgraduate programme. There are no previous studies on this subject reported in the literature from India, however, the surgical training programme have been undergoing changes in USA and UK. It has probably existed in our country because of lack of quality control audits of surgical outcomes[5] that are commonly practiced in other countries. The present system as laid down by the MCI, states that the learning in residency should be autonomous and self-directed. There should be adequate exposure to community-based activities and to human behavior. The assessment of the student should be both summative and formative. The current assessment is based on one time examination at the place of training at the end of the training programme which lasts three years.[1] The thesis component of the training programme is expected to educate the trainee on the concepts of research methodology and epidemiology and make them capable to critically analyze published research literature. It is also expected that during the residency the trainee comes up with genuine research. There are often eyebrows raised on the genuineness of the research deserted by the residents. It is considered to be a formality that is just fulfilled and done away with. The opinion expressed on this aspect was that the thesis programme is an important part of learning experience but changes must be made in its evaluation and better tools and infra structure for research in the institutions should be provided. Some have suggested that one or two publications rather than a thesis should be in the curriculum as a more appropriate method of improving research in the field of surgery as it is more critically scrutinized in peer reviewed journals. The publications, however, cannot be mandated because of time bound completion of MS surgery programme. A publication may take long time to mature however completion of one or two intramural projects may be considered as an alternative of writing and publishing thesis. A surgeon is expected to be an effective leader of a health team engaged in providing health care.[1] Grande and Volpp advocated the idea of team approach and the creation of collegial culture that encourages reporting an adverse event to improve patient safety, an issue assuming greater importance in the present society.[6] The trainee should also acquire adequate communication and administrative skills during the residency. The present system offers little for the trainee to harness these skills and no courses or lectures on this aspect are offered to most trainees. The results in our study favor that teaching of leadership skills should also be a part of the new curriculum. The hectic work schedule of the residents has often made the education component of the residency programme take a back seat sometimes compromising the competence of the residents. In many medical institutions, the duties of the residents include transporting patients, withdrawing blood samples, filling laboratory forms and several such service functions that can easily be done by paramedical staff. If the workload is shared by reinforcing paramedical staff and other services, the resident may better utilize his/her time in studying, doing research or doing preparation for the next day elective surgery by reviewing records and reviewing literature of the patients pathology and going through relevant text and pertinent journal articles. An untired and well-prepared resident would find the operating room experience more rewarding. The acquisition of knowledge can be autonomous and self-directed, however, postgraduate teaching by experienced surgeons go a long way in kindling the desire in the trainee to achieve more. It can lay down a sound foundation on which each individual can build upon to have more thorough and updated knowledge. The present system needs more experienced teachers with an academic mindset and greater number of teaching hours to achieve the above goals. Surgery is a great blend of theoretical knowledge, operating skills and lots of interpersonal skills. It is often said that skills can be best acquired when transferred from one experienced surgeon to a young enthusiastic surgeon by personal contact. The Guru-Shishya ( mentor-mentee ) system practiced in India from old times may offer the best way of transferring skills to the trainee because it brings passion rather the profession in imparting the operating skills. The mentor is the person who encourages, cajoles, and compassionately stimulates the student to achieve necessary skill to become an independent practitioner in surgery. The current random nature of accruing procedural and patient care skills is inconsistent with studies demonstrating that acquiring skills needs 'deliberate practice.'[7] There should be ideal mix of supervision and independence for surgical skill to bud and blossom. The newer system should lay down criterion of minimum number of surgery in which the trainee should assist senior surgeons and also the senior surgeon to assist the trainee. There is no emphasis on use of modern technology in improving surgical skills in the trainees. The surgical skills laboratories have provided evidence that indeed use of simulators and trainers improved skills and improve operating room performances.[8] Often voices have been raised against the evaluation and examination in the present residency programme. Examination is usually conducted at the place of training and mainly by in house examiners with a couple of external examiners. There is provision of one time examination at the end of the training programme. While evaluating trainee for masters in surgery, surgical skills are never tested and so is the non-evaluation of mannerism of the trainee or this attitude and behavior towards the patients. The administrative, communication and interpersonal skills are generally not tested during the examination. Most residents get the education piece mostly as a function of being in the hospital for so long. Some studies conducted in USA have shown that the evaluation system meant nothing more than the individual had fulfilled a minimum set of requirements and had passed a written and oral examination and have failed to address the issue of competence or quality of the education.[9] It would be naοve to assume that time alone, i.e., 3 years programme will make all residents equally competent to practice surgery. Obviously, not all residents develop surgical skills at same rate. The system has no means in identifying such students and therefore cannot offer individualized attention to such residents. The residents advance in the course merely by completion of the specified time and not tied to demonstration of competence. It may be difficult to implement such a differential in training programme, and it requires a major national debate. General surgery, is truly a specialty contrary to what the name suggests[10] and this fact need be re-emphasized and re-established especially in the time where most sub-specialty have taken up the band wagon of 'superspeciality.' General surgery is the tree from which these branches of sub-specialties have taken origin. It is ironical some have questioned the place of general surgeons in the coming future and also advocated an early dichotomy from the basic surgical training. It is certain that general surgery would keep on mothering newer sub-specialties such as rural surgery, minimal invasive surgery, and so on, but keep on producing newer, more skilled and more competent surgeon-scientists and surgeon-epidemiologists if carefully engineered changes are made today and a dynamic system is created taking regular feedbacks from students and teachers. The changes made today would require validation by closely following and scrutinizing the results in the future. The results should be in the right direction to justify these changes in the residency programme. This study raises few issues about the common experiences, which all general surgeons share during surgical residency programme today. More studies in this vast field of medical education are probably needed in India to investigate in detail various aspects of the surgical residency programme. These studies should take into consideration the variation in language, culture, and customs for a vast country like India. In view of above the external validity of this study may be limited to northern states and may not represent the views of other institutions in the country. Similar studies and even more broad based study may be required in southern or whole of India in representative sample. This could be an ideal investment now to build a better future for newer generations of general surgeons. The open-ended views expressed by most teachers and resident responders can be summarizing as follows. Stereotype training in surgery can no longer be acceptable firstly because of increase in knowledge and emergence of new technologies, e.g., laparoscopic and video-endoscopic surgeries and secondly, due to changing social and economic situation and higher expectations of the patients. Thirdly and perhaps most importantly, the very existence of the departments of general surgery appears to be challenged by emergence of various sub-specialties like cardiac surgery, neurosurgery, and pediatric surgery, etc. leading a void and need for much intensive general surgical teaching and training with the broad base of clinical epidemiology, pre-hospital care, trauma, critical care, microvascular surgery, minimally accessible surgery, wound care, public health aspect of general surgery, human ethics, and research methodology, etc. In view of inclusion of these topics in MS curriculum the duration of the course should be extended to a period of 5 or 6 years and at the conclusion of 5 year course, a sub-speciality MCh degree in general surgery should be awarded atleast in some institutions and on some seats to prepare academic general surgical teachers. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06090t1.jpg] |
| |||||||||

{kind=link}