 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
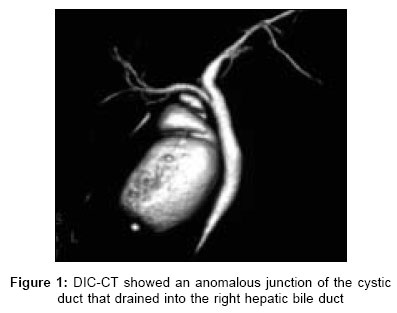
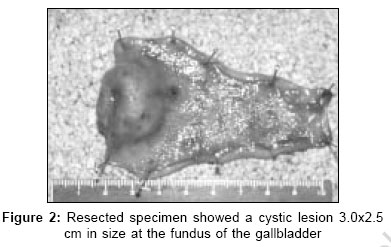
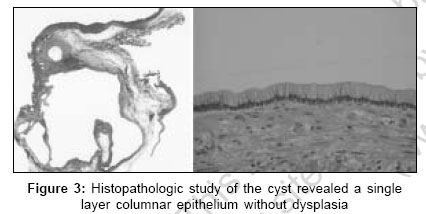
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 316-317 Case Report Gallbladder cyst with an anomalous junction of the cystic duct Hirano Yasumitsu, Tatsuzawa Yasuhiko, Shimizu Junzo, Kawaura Yukimitsu, Ishikawa Norihiko, Watanabe Go Department of Surgery, Saiseikai Kanazawa Hospital, Ni 13-6, Akatsuchi-machi, Kanazawa 920-0353; Department of General and Cardiothoracic Surgery, Kanazawa University, Graduate School of Medical Science, 13-1, Takara-machi, Kanazawa 920-8641 Code Number: is06091 Abstract Gallbladder cyst is a rare entity. We herein report a case of gallbladder cyst with an anomalous junction of the cystic duct and review the literature. A 49-year-old woman was admitted to our hospital with cholecystolithiasis. Computed tomography (CT) and ultrasonography showed a few stones in the gallbladder. Multi-slice CT cholangiography showed an anomalous junction of the cystic duct which drained into the right hepatic bile duct. At surgery, a smooth mass-like lesion was noted at the fundus of the gallbladder. Laparoscopic cholecystectomy was performed without bile duct injury owing to the preoperative information on the cystic duct. The resected specimen showed a cystic lesion 3.0x2.5 cm in size at the fundus of the gallbladder filled with colorless mucus. Histopathologically, the inner surface of the cyst was lined by a single layer of columnar epithelium without dysplasia.Keywords: Anomalous junction, gallbladder cyst, multi-slice computed tomography cholangiography Introduction Gallbladder cyst is a rare clinical entity. We experienced a patient with gallbladder cyst combined with an anomalous junction of the cystic duct and treated laparoscopically without perioperative complications using multi-slice computed tomography (CT) cholangiography for preoperative examination.Case Report A 49-year-old woman was admitted with a two-year history of cholecystolithiasis. She had a past history of appendectomy 33 years prior to admission. On admission, she was well and her blood analyses were all normal. CT and ultrasonography of the abdomen showed a few stones in the gallbladder. Magnetic resonance cholangiography revealed no common bile duct (CBD) stones. Multi-slice CT cholangiography (DIC-CT) showed an anomalous junction of the cystic duct which drained into the right hepatic bile duct [Figure - 1]. Under a diagnosis of cholecystolithiasis with an anomalous junction of the cystic duct, laparoscopic surgery was performed. At surgery, a smooth mass-like lesion was pointed out at the fundus of the gallbladder. We performed laparoscopic cholecystectomy (LC) in the usual fashion because the mass-like lesion had no serosal invasion and was free from the liver bed. Intraoperative cholangiography was carried out to confirm that the right hepatic bile duct was intact. The resected specimen showed a cystic lesion 3.0x2.5 cm in size at the fundus of the gallbladder, filled with colorless mucus [Figure - 2]. Histopathologically, the inner surface of the cyst was lined by a single layer of columnar epithelium without dysplasia [Figure - 3]. The postoperative course was uneventful and she was discharged five days postoperatively.Discussion Gallbladder cyst is rare. The first case of this unusual entity was reported by Wiedemann in 1797 as an elongated mass containing a whitish cheese-like substance.[1] The etiology of gallbladder cyst is unknown, but various hypotheses have been represented for the possible cause of cyst formation.[2] The majority of gallbladder cysts are usually related to the Rokitansky-Ashoff sinus. They contain mucin-like fluid, bile pigments, cholesterol crystals and even typical gallstones and are usually associated with chronic inflammation of the gallbladder and frequently with the presence of stones.[3] From these facts, we suspected that gallbladder cyst may result from the partial or complete closure of the outlet of the pseudodiverticulum, such as the Rokitansky-Ashoff sinus, by an inflammatory or neoplastic process. Fourteen cases with gallbladder cyst have been documented in the world literature, according to Medline.[2],[4],[5] Including the present case, 11 cysts were at the fundus of the gallbladder and another two cases at the body. The majority of these were less than 3 cm in diameter. The contents of the cyst varied from mucus, serous fluid, bile pigments, cholesterol crystals and even typical gallstones. Two cases of cysts (14.2%) included atypical cells in histopathological examination and this indicated the possibility of malignancy arising from these cysts. Surgical resection of the gallbladder should be performed because no definite strategy for gallbladder cysts had been established. Anatomic variations of the cystic duct are seen in about 2% of cases, which require careful observation at the time of operation to avoid injuring other structures. laparoscopic cholecystectomy is known to be safe and has gained acceptance as a standard procedure. Clear biliary tract imaging prior to the operation is essential to safely performing LC. Takeuchi et al[6] reported the efficacy of DIC-CT and concluded that DIC-CT provides an advantage in relation to operative time, conversion and procedure-related perioperative complications. We have routinely employed DIC-CT as a preoperative examination for LC since October 2002. In the present case, DIC-CT showed an anomalous junction of the cystic duct, which drained into the right hepatic bile duct. Owing to this information, we safely performed LC without any intraoperative complications. We experienced an unusual case of a patient with gallbladder cyst combined with an anomalous junction of the cystic duct. It is hard to comment on the clinical significance of this cyst and bile duct anomaly, which we discovered accidentally. However, some such cysts include atypical cells, so surgical resection of the gallbladder should be performed and DIC-CT is a useful and necessary examination for evaluating anomalous bile ducts before LC. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06091f3.jpg] [is06091f2.jpg] [is06091f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}