 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
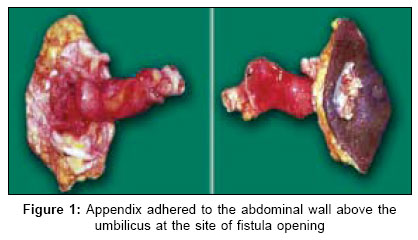
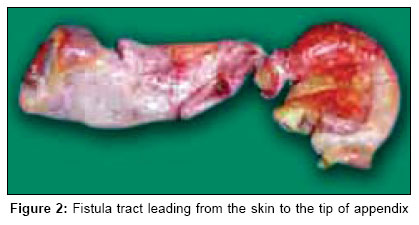
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 318-319 Case Report Appendico-cutaneous fistula Muthukumarassamy R, Shankar R, Sistla S, Jagdish S Department of General Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry Code Number: is06092 Abstract One of the rare complications of appendicitis is the formation of fistulous communication between appendix and adjacent viscera or skin. We report three unusual cases of cutaneous fistula that developed following acute appendicitis. Symptoms at presentation and pathogenesis of the unusual lesions are reviewed. Various diagnostic modalities-skiagram, ultrasonogram and sinogram are discussed. Appendicetomy is the treatment of choice when the diagnosis is usually made.Keywords: Appendicitis, appendix, sinus Introduction Appendicular fistula, an uncommon complication of acute appendicitis is the most uncommon type of enteric fistulas. Various types of fistulous communication reported are appendicovesical, appendicointestinal, appendicouterine and appendicocutaneous.[1] An appendiceal fistula is formed by the spontaneous perforation of appendix to adjacent hollow viscera such as the urinary bladder or the bowel or to the abdominal wall or skin. Although appendicovesical and appendicointestinal fistula are rare, appendicocutaneous fistula is even more infrequent and offers diagnostic challenge as cause of fistula.[2],[3] Reviewing literature by Medline search, we found that only six case reports of appendicocutaneous fistula to date (nine cases).[4] We present the various presentation of the rarest form enteric fistula and discuss the management of the appendicocutaneous fistulas.Case reports Case 1 A 60-year-old man was admitted with complaints of right iliac fossa (RIF) pain with tenderness and guarding. He was diagnosed as acute appendicitis and managed conservatively with IV antibiotics. He presented four months later with history of pus discharge from the right flank, which started as an acute swelling and ruptured discharging pus. On examination, a sinus discharging pus was found in the right lateral abdominal wall and no mass was palpable. Sinogram revealed an abscess cavity without any communication to the bowel. Exploration under general anesthesia showed a fistula connecting skin, an abscess cavity and tip appendix. Excision of the fistula along with appendix was done. Histopathological examination showed chronic appendicitis with a non-specific inflammatory tract. Case 2 A 19-year-old boy presented with acute onset of swelling in the periumbilical region, which ruptured and started discharging pus and faeces after two days. He had been admitted two weeks earlier with history of acute RIF pain with tenderness during which he was diagnosed as acute appendicitis and was managed conservatively. On examination, a sinus was seen above the umbilicus discharging fecal matter along with pus. Fistulography showed a fistula communicating with the bowel. The fistula was explored under general anesthesia when the discharge decreased. There was a fistulous tract leading to the tip of appendix from the skin above the umbilicus and excision of tract along appendix was done [Figure - 1]. Histopathological examination showed chronic appendicitis with a fistula. Case 3 A 67-year-old lady presented with history of persistent fecal discharge from the RIF at site of previous surgery. She had undergone drainage of suspected right psoas abscess in a clinic and in the immediate postoperative period she had fecal discharge from the incision site and a defunctioning ileostomy had been done. On examination at our hospital, she had a functioning ileostomy and a fecal discharge from the transverse scar in the RIF. Biopsy from the fistula opening was done which showed chronic inflammatory granulation with no evidence of tuberculosis. Ileostomy was closed when the discharge settled. The patient presented two years later with incisional hernia and persistent purulent discharge from the fistula site. On exploration, the fistula tract of 2 cm length was found extending up to the summit of the appendix [Figure - 2] and so the fistula along with the appendix was excised with repair of incisional hernia. Histopathological examination revealed a fistulous tract with chronic appendicitis. Discussion Spontaneous appendicocutaneous fistulas are rare complications of untreated appendicitis. According to Kjellman, the main mechanism of formation of the fistula is the spontaneous rupture of inflamed appendix into the adjacent bowel or the skin and persistence of fistula is due to the presence of appendiceal calculus or carcinoid tumor or tuberculosis.[3],[4] In these three cases appendicoliths were not identified and probably were discharged initially along with the pus and persistence of the fistula was due to the epithelization of the tract. Most of the fistulas appeared as subcutaneous abscess which when ruptured or drained persisted as non-healing sinus. The fistula tends to heal with slight pus or mucinous discharge, which may explain the absence of communication with bowel on sinogram or barium enema. Rarely, the tract is big and these patients present with fecal fistula and typical communication from skin to caecum can be seen in the sinogram.[3] Presence of appendicoliths, on plain abdominal roentgenogram, may provide the vital information for diagnosing the appendicocutaneous fistula in the absence of fistulous communication with the caecum. Appendicocutaneous fistula is diagnosed by ultrasonogram of abdomen - to assess the extent of abscess and water-soluble contrast sinogram. Early treatment by excising the fistulous tract along with appendix is the preferred modality of management as shown in our series.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06092f2.jpg] [is06092f1.jpg] |
| |||||||||

{kind=link}
{kind=link}