 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
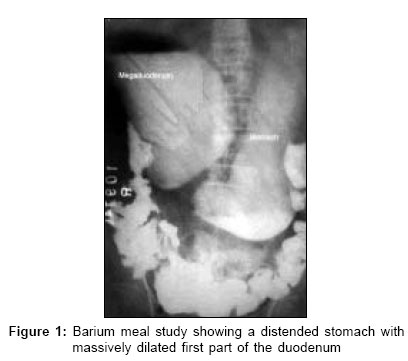
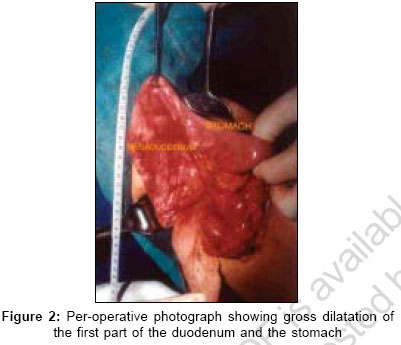
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 320-321 Case Report Mega-duodenum due to isolated segmental duodenal aganglionosis Barmeda ShaileshH, Porecha MehulM, Bhimbhara PanchampalS, Mehta PurviJ, Vasavada HiralD, Sharma NirajJ Department of Surgery, M. P. Shah Medical College, Guru Gobind Singh Hospital, Jamnagar, Gujarat Code Number: is06093 Abstract Isolated segmental duodenal aganglionosis is an extremely rare condition. We report a case of mega-duodenum due to an isolated aganglionic segment in the second part of the duodenum. A 60-year-old female presented with a history of off-and-on non-bilious vomiting and upper abdominal fullness after each meal. Investigations suggested that the stomach and the first part of the duodenum were grossly dilated. On exploration, a narrowed segment in the second part of the duodenum with gross dilation of the proximal duodenum and the stomach was found. Retrocolic duodenojejunostomy was done and a biopsy was taken from the narrowed duodenal segment. Histopathology examination revealed near-complete absence of the ganglion cells in the narrowed segment.Keywords: Aganglionosis, double bubble appearance, duodenojejunostomy, mega-duodenum Introduction Mega-duodenum is a huge dilatation of duodenum. The causes of mega-duodenum are superior mesenteric artery syndrome, congenital duodenal atresia, annular pancreas, systemic sclerosis and visceral myopathy. However, mega-duodenum due to duodenal aganglionosis is an unusual condition and isolated segmental duodenal aganglionosis is extremely rare.[1] Very few such cases have been reported.Case report A 60-year-old female presented with a history of fullness of upper abdomen after each meal since 12 years. It was associated with off-and-on non-bilious vomiting of ingested food particles. On examination, she was found to be malnourished and she had upper abdominal distention. The erect abdominal radiograph surprisingly revealed 'double-bubble' appearance, which is usually seen in duodenal atresia in neonates. Barium meal study showed a distended stomach with massively dilated first part of the duodenum [Figure - 1]. Passage of barium through the second part of the duodenum was very slow and the stomach and first part of the duodenum showed significant barium residue even after 24h. Passage of barium through rest of the bowel was normal. Ultrasonography and computed tomography examination suggested grossly dilated stomach and first part of the duodenum. Other abdominal organs were normal. Upper GI endoscopy confirmed the dilatation with smooth negotiation of scope in the second part of the duodenum and absence of any ulcer or growth. On abdominal exploration, gross dilatation of the stomach and fusiform dilatation of the first part of the duodenum were found [Figure - 2]. Just beyond the dilatation, there was a 3 cm long narrowed segment in the second part of the duodenum. No evidence of any inflammation, scarring or growth, periduodenal adhesions or enlarged lymph nodes was found. The pancreas, rest of the intestines and other viscera were normal. Dilated duodenum was mobilized, opened and examined. There was no intraluminal pathology and its wall was hypertrophied. Full-thickness biopsy was taken from the wall of the narrowed segment. Side-to-side retrocolic isoperistaltic duodenojejunostomy was performed between the dilated first part of the duodenum and the proximal jejunal loop, 12 cm from the duodenojejunal flexure. Postoperative course was uneventful and patient was relieved of her symptoms. Histopathology examination was reported as 'near-complete absence of ganglion cells in the second part of the duodenum.' Barium meal study performed after six weeks of the surgery showed smooth passage of barium through the anastomosis and normal emptying of the stomach and the duodenum. Discussion Mega-duodenum due to aganglionosis is very unusual. Aganglionosis of the bowel is an intestinal neuromuscular disorder in which there is an absence of ganglionic cells in the myenteric plexus. Proposed etiological theories are congenital disorder of migration of neuroblasts and acquired ischemia of the bowel.[2] Most of the patients present in infancy and childhood but in 7 to 8% of cases, diagnosis is delayed till adulthood.[3] Presentation in old age is extremely rare. Hirschprung's disease is the most common intestinal neuromuscular disorder in which aganglionic segment is located in the anal canal, rectum and a variable part of the large intestine. Total aganglionosis of the gastrointestinal tract is rare and is associated with small bowel involvement in 70% cases.[4] Abnormal motility of duodenum and esophagus has been reported in Hirschprung's disease and there have also been reports of mega-duodenum and mega-colon in the same patient.[2],[5] Isolated segmental duodenal aganglionosis is extremely rare. The first authentic report of the same is by Sulaiman et al in which the patient was an adult having a 6 cm long aganglionic segment immediately beyond the pylorus and acquired segmental ischemia was considered as an etiology.[1] The second case was reported by Puri et al in which the patient was an adult having aganglionic segment in the third and fourth part of the duodenum, which was associated with bowel malrotation and congenital etiology was considered.[6] In our case, the patient was a 60-year-old female having aganglionic segment in the second part of the duodenum. Considering the age of the patient and absence of congenital anomaly, acquired segmental ischemia is the suspected etiology. Here we have performed duodenojejunostomy because it is the treatment of choice in duodenal atresia in the newborn.[7] Second reason is that we have already opened up and mobilized the dilated duodenum to rule out intraluminal pathology, so it is now fairly justified to do duodenojejunostomy instead of gastrojejunostomy; however, one can do gastrojejunostomy in such type of cases. It should be emphasized that in cases of megaduodenum, aganglionosis, though rare, should also be considered a probable etiology. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06093f2.jpg] [is06093f1.jpg] |
| |||||||||

{kind=link}
{kind=link}