 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
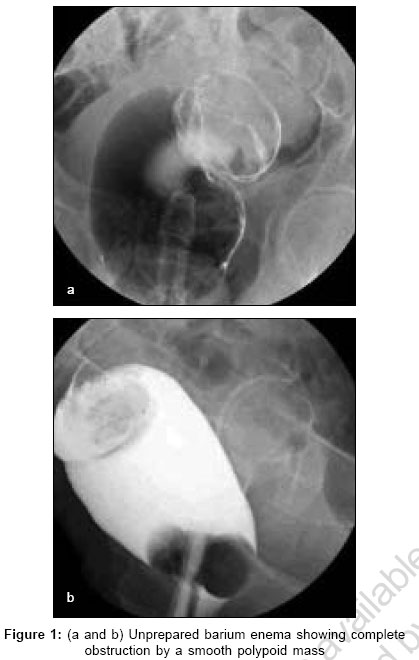
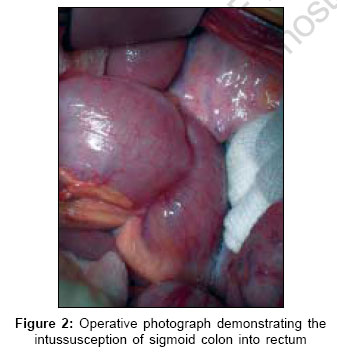
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 322-324 Case Report Colonic intussusception in adults: Three cases and review of the literature Garner JeffreyP, Haldipur Nandan, Ravi Krish, Amarnath TakalokoppaS, Gupta Robin Department of Colorectal Surgery, Chesterfield and North Derbyshire Royal Hospital, Calow, North Derbyshire S44 5BL Code Number: is06094 Abstract Adult intussusception is a different disease from that encountered in children with a higher rate of pathological lead points, the majority of which in the colon are malignant. This has supported a practice of mandatory laparotomy and en bloc resection without reduction for colonic adult intussusception. We report three cases of adult colonic intussusception, which demonstrate a variety of presenting features and discuss the investigation and treatment of this uncommon condition.Keywords: Adult, colonic, intussusception, obstruction Introduction Intussusception in adults is much less common than the childhood variant with markedly different aetiologies and presentations; the literature contains several hundred adult cases,[1] yet many surgeons will never have seen a single case and it may not be considered in the differential diagnosis of recurrent intermittent abdominal pain or acute intestinal obstruction.[2] There is a pathological lead point in 90% of adult cases and most involve only the small bowel (enteric type) or are ileocolonic.[3] In the colon, right-sided lesions predominate and the incidence of a malignant intussusceptum is approximately three times higher than in the small bowel[4] - consequently pre-or intra-operative reduction has traditionally been eschewed in favour of en bloc resection.[5] We report three cases of adult intussusception involving the left colon which demonstrate the range of presenting features of the condition and some of the diagnostic and therapeutic dilemmas that may arise.Case Reports Case 1 A 72-year-old man presented with a 10-day history of absolute constipation, lower abdominal pain and bright red rectal bleeding. He described obstructed defecation and a lump coming down prior to this and was clinically anaemic. Abdominal examination was unremarkable but digital rectal examination revealed a smooth bulbous swelling at the fingertip suggestive of a polypoid lesion. An unprepared barium enema revealed complete colonic obstruction from a polypoid rectal mass [Figure - 1] a and b consistent with colorectal intussusception. At laparotomy colorectal intussusception was confirmed [Figure - 2] and after manual reduction of the intussusception from the above, he underwent Hartmanns procedure as the distal rectum was too oedematous to allow primary anastomosis. His post-operative course was unremarkable and histological examination confirmed a pT 3 N 0 M x colonic adenocarcinoma as the lead point of his intussusception. Case 2 A 51-year-old lady presented as an emergency with one month of severe left lower quadrant pain associated with 10 days of absolute constipation. She had suffered for many years with intermittent low abdominal pain associated with constipation, abdominal distension and borborygmi, which would settle spontaneously after a few days. Plain abdominal X-ray demonstrated colonic obstruction and urgent contrast enema confirmed almost complete obstruction by suspected tumour. Laparotomy revealed a bulky sigmoid tumour; because of gross colonic obstruction she underwent Hartmanns procedure. Histology demonstrated her 'tumour' to be an unsuspected colonic intussusception with no obvious lead point in an area of complex diverticulosis. There was no evidence of neoplasia. Case 3 A 50-year-old lady was admitted acutely with a large rectal mass prolapsing through the anus and one month of constipation but no other gastrointestinal symptoms. Bedside examination revealed a large polypoid lesion protruding from the anus, which unfortunately reduced itself under general anaesthetic and could not be snared at sigmoidoscopy. The following day rectal examination was unremarkable but five days later an easily palpable smooth rectal mass was again evident with the patient complaining of significant perineal and abdominal discomfort. Unprepared barium enema demonstrated a smooth 10 cm rectal mass with complete obstruction suggesting intussusception. The patient was scheduled for emergency anterior resection when she spontaneously passed a polyp per rectum with complete resolution of her symptoms. Histological examination confirmed the lesion to be a large, simple polypoid lipoma and subsequent sigmoidoscopy confirmed normal colonic mucosa. Discussion Adult intussusception is a different entity to the childhood condition. It is much less common, accounting for only about 3% of cases of obstruction in most series[6] and has an identifiable pathological lead point in up to 90%[1] of cases in stark contrast to paediatric presentations. Few case series contain more than 50 patients collected over several years reflecting its relative rarity. The majority are enteric or ileocolic cases, with only one third of adult intussusceptions being colocolic or colorectal in nature.[1] Colonic intussusceptions have a much higher rate of lead point malignancy than enteric ones, with approximately two thirds of colonic cases having a malignant basis compared to one quarter of enteric types;[1],[4] anaemia at presentation and anatomical location within the colon are independent predictors of malignancy[1] and it is this, that underpins the recommendation that colonic intussusceptions should be resected en bloc without reduction. Acute presentations represent only about 14% of cases, with the duration of symptoms usually exceeding one month[4] and in many cases extending over many years - it is likely that our second case had been having bouts of intermittent intussusception over several years accounting for her intermittent self-limiting distension, borborygmi and constipation. The findings on presentation are those of large bowel obstruction - a palpable mass is rarely present. Investigations are directed at confirmation of obstruction followed by elucidation of the cause. A plain abdominal film is useful only for the first reason whereas contrast enema confirms obstruction in 95% of cases and suggests intussusception as the reason in approximately 50% of cases,[2],[4] although two out of three of our cases were correctly identified by contrast enema. Ultrasonography has only recently begun to be used for this condition and diagnostic features such as the 'concentric ring' sign are described. The limited evidence to date suggests it is highly accurate, correctly diagnosing all nine patients in one small series.[7] Computed tomography (CT) scanning is the investigation of choice with an accuracy approaching 100% for modern scanners - the intussusception appears as a sausage shaped mass on longitudinal section and as a 'target lesion' on cross section. The CT scan also delivers important staging information in malignant cases.[8] Half fourier single shot turbo spin echo (HASTE) sequence magnetic resonance imaging scanning has been used in the assessment of bowel obstruction and intussusception with good success but is not often readily available, has significant contraindications and in colonic obstruction is more difficult to interpret than CT scanning - it is not therefore recommended as a first line investigation.[9] The diagnosis can be made at colonoscopy where direct inspection reveals a mushroom-shaped lesion filling the lumen - it also allows histological diagnosis of the lesion to better inform the operative decision making.[10] The standard treatment of adult colonic intussusception is resection; debate however centres around the potential role of reduction prior to resection. The high incidence of malignant lead points in colonic intussusception has led to a widespread adoption of a policy of resection en bloc to minimise potential tumour seeding.[2] For sigmoidorectal intussusception however this may necessitate acute abdominoperineal resection and permanent end colostomy. In this circumstance several authors have suggested that reduction prior to resection may be permissible. Weilbacher[5] suggested obtaining a histological diagnosis of the lead point before resection: malignant leads without evidence of metastases should be resected en bloc but those with metastases or benign lead points should be reduced first to allow low anterior resection. The colonic resection may be performed laparoscopically following standard oncological parameters and the laparoscopic instruments may be used to reduce the intussusception if desired with or without manual assistance per rectum,[11] alternatively diagnostic laparoscopy may be used to identify the intussusception although the diagnosis should be obtainable by a combination of the non-invasive methods described. Sarr proposed that all adult intussusceptions should be reduced either colonoscopically or hydrostatically to convert an emergency operation on obstructed colon into an elective one on 'prepared' bowel, to decrease the rate of end stoma formation as the distal colon is often too oedematous to safely permit primary anastomosis as in our cases.[12] Adult intussusception is an uncommon condition but remains an important differential diagnosis in cases of intermittent bowel obstruction or those presenting with acutely with complete obstruction. There is increasing evidence that small bowel and colonic intussusceptions can be managed differently and efforts should be made to optimally characterise both the intussusception and likely lead point. CT scanning is the single most useful investigation for colonic cases, whilst colonoscopy allows a preoperative histological diagnosis of the lead point. Resectional surgery without reduction remains the mainstay of treatment of colonic intussusception, given the high incidence of malignant lead points, but consideration should be given to attempting reduction to allow either delayed elective surgery or avoidance of an abdominoperineal resection. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06094f2.jpg] [is06094f1.jpg] |
| |||||||||

{kind=link}
{kind=link}