 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
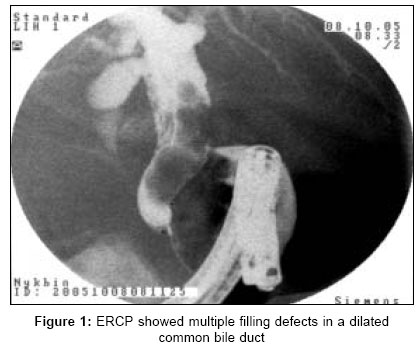
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 328-329 Case Report Delayed cholangitis due to a retained T-tube fragment Kourosh Shamimi, Fereydon Moazami, Mehdi Jalali, Ali Aminian Department of General Surgery, Tehran University of Medical Sciences, Tehran Code Number: is06096 Abstract Biliary drainage with T-tube after bile duct exploration has some advantages. However, the use of T-tube is associated with significant complications. Retained T-tube fragment is a rare complication after biliary surgery. We present an unusual case of delayed cholangitis resulting from a retained T-tube fragment and common bile duct stones, occurring four years after previous bile duct exploration in the case of colon cancer. We recommend early removal of a missing fragment to avoid potential serious complications. Keywords: Cholangitis, choledochotomy, common bile duct, complication, T-tube Introduction T-tube is commonly used in patients after complex biliary surgery when a choledochotomy is performed. The rationale for the use of T-tubes is to ensure biliary decompression, permit healing of the choledochotomy and to create a tract lined by granulation and fibrous tissue. It minimizes bile leakage, provides access for cholangiography and removes occasional retained stones. But the use of T-tubes also has been associated with significant complications. One such rare complication is a retained T-tube fragment.[1],[2] Only five cases have been reported previously in English literature.[3],[4],[5],[6],[7] We report an unusual case of cholangitis caused by a T-tube fragment and common bile duct stones, occurring four years after bile duct exploration.Case report A 45-year-old man was transferred from gastroenterology unit to our service because of acute cholangitis and failed endoscopic sphinctrotomy. He was operated four years ago because of colon cancer and he received adjuvant chemoradiotherapy. He was relatively well until three months prior to admission, when he developed progressive jaundice, intermittent fever and right upper quadrant pain. He was admitted with the impression of acute cholangitis. Liver tests were in favor of obstructive jaundice. Abdominal sonography and computed tomography scan showed multiple gallstones, dilated common bile duct (CBD) with large stones and no clear evidence of residual malignancy. Following initiation of medical management including antibiotic therapy, ERCP was done [Figure - 1]. Endoscopic sphinctrotomy was attempted but failed, so he was transferred to our surgical unit for bile duct exploration. At operation, there was no evidence of intra-abdominal malignancy. There were some adhesions in right upper quadrant, which was released. CBD was dilated. After cholecystectomy, choledochotomy was performed. After removal of multiple biliary stones, we surprisingly noticed the "T" fragment of the T-tube in the CBD. We closed the CBD over a new T-tube. Postoperative recovery was uneventful. T-tube cholangiography at 13th postoperative day revealed no obstruction, so the T-tube was removed one day later. He was discharged in good condition. Review of his previous admission records showed that he had a colo-duodenal fistula caused by direct tumoral invasion; therefore, he underwent extended right colectomy with removal of the involved portion of duodenum and a T-tube was inserted for the protection of duodenal repair. However, in the postoperative period, "T" fragment of T-tube was separated and retained at the time of removal. He was asymptomatic during these years. Discussion Many complications have been reported with T-tubes. The most common complication at the time of removal is bile leakage. Other complications include cholangitis, T-tube dislodgment or occlusion and fluid and electrolyte imbalance. Bile duct traumas during removal, bile leakage leading to peritonitis, retention of a fragment and stricture formation after removal have also been reported.[1],[2] Retained T-tube fragments are actually a very rare complication; indeed, in the English literature, only few case reports are mentioned about this complication.[3],[4],[5],[6],[7] Among the five cases previously reported, three T-tubes were withdrawn endoscopically, one surgically and one by a balloon dilatation catheter coaxially inserted within the retained broken fragment.[3],[4],[5],[6],[7] In addition to theses case reports, only one study mentions a single retained T-tube among a series of 274 cholecystectomies with choledochotomy.[1] Although recommendations for the optimal time for T-tube removal are two weeks after choledochotomies and three months after liver transplantation, there is no clear evidence that leaving a T-tube in the biliary tree for prolonged period could elicit a fibrous reaction responsible for retaining the tube.[2] Recently Ojanguren et al reported a simple method for removal of intact T-tubes that could not be removed by a standard manual traction to prevent separation and missing of T-tubes. They recommended use of a balloon with a diameter 20 to 25% larger than the T-tube diameter. As the balloon is dilated to its inherent diameter within the T-tube, it breaks the adhesions between the tube and the fistulous tract. This frees the T-tube and prevents separation of T-tube with excessive manual traction.[8] Despite the declining numbers of bile duct explorations in the laparoscopic era and the tendency to carry out primary closure of a choledochotomy, the T-tube will continue to be a useful tool in biliary surgery. We emphasize on the importance of careful tube preparation at the time of insertion, use of percutaneous dilatation technique after failed manual traction of tube to prevent separation and finally early extraction of a missing fragment to avoid potential serious complications. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06096f1.jpg] |
| |||||||||

{kind=link}