 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
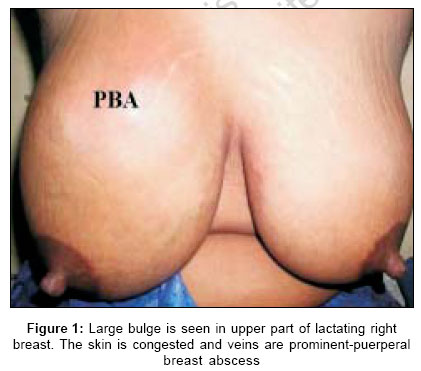
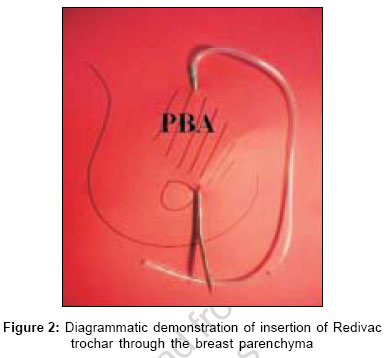
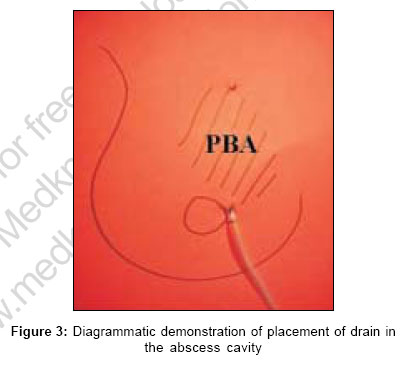
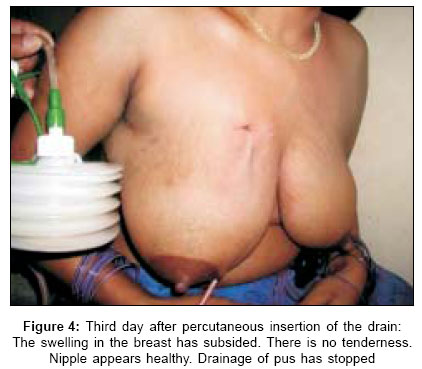
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 330-333 Point of technique An effective method of drainage of puerperal breast abscess by percutaneous placement of suction drain Tewari Mallika, Shukla HS Department of Surgical Oncology, Institute of Medical Sciences, Banaras Hindu University, Varanasi Code Number: is06097 Abstract We present a new minimally invasive method of percutaneous placement of suction catheter in patients of puerperal breast abscess (PBA). 30 patients between 18 and 34 years of age were treated by this novel technique from January 1999 to January 2005 after an informed consent. Among them there were primi-para 15, 2nd para 10 and 3rd para 5 lactating mothers. Clinical diagnosis of PBA was based on history and presence of tender fluctuant abscess in the breast. The treatment was carried out on presentation in the outpatient department. Under local, 0.5% lignocaine with adrenaline, infiltration anesthesia 16F suction catheter was placed percutaneously in the abscess cavity for 3-8 days. Results: The abscess healed in 5-8 days time. There was no complication of residual or recurrent breast abscess, fistula or sinus formation, induration or distortion of the breast parenchyma. There was no scar formation. Breast-feeding was not interrupted in any patient.Keywords: Breast feeding, drainage of breast abscess, puerperal breast abscess Introduction Drainage of puerperal breast abscess (PBA) has undergone a gradual change from invasive to minimally invasive procedure in keeping with the current philosophy of surgery. The standard surgical approach (invasive) of incision and drainage (I and D), breaking of loculi and insertion of a drain under general anesthesia[1] or daily gauze packing[2] has yielded to minimally invasive approach of aspiration/repeated aspiration of the abscess in the radiology department under ultrasonic (US) guidance.[3] The I and D method requires hospitalization, surgical facilities and entails certain morbidity and cessation of breast function. The minimally invasive method requires presence of an invasive radiology department. We describe here a minimally invasive, effective method of drainage of breast abscess that does not require hospitalization or ultrasonographic facilities. Materials And Methods Thirty patients with large fluctuant PBA were treated by this technique from January 1999 to January 2005. Age ranged from 18 to 34 years. An informed consent was obtained from each patient prior to the procedure. 15 patients were primi-para, 10 para-2 and 5 were para-3 lactating mothers. Patients generally presented with a history of fever and pain in either breast for past few days and had been on antibiotics and analgesics. Examination revealed a large diffuse bulge in the affected breast that was tender and fluctuation was present. A diagnosis of PBA was thus made and confirmed on needle aspiration. The drainage of breast abscess was carried out in the out patients department on first attendance. No preparation other than measurement of vital functions and random blood sugar and full blood count by finger prick method was required. Patient was explained the procedure and an informed consent taken. In supine position in the minor operation theatre, annexed to the outpatient department the abscess was drained by the following method: The patient shown [Figure - 1] had large fluctuant PBA in the upper half of right breast. Lignocain (with adrenaline in 0.5% strength) local infiltration anesthesia was given 2 cm above the upper palpable margin of the abscess and at areola-skin junction at 3' clock position for entry and exit of the suction drain trochar, respectively. Number 16F trochar of suction drain was inserted at the upper edge and brought out through the abscess cavity, at 3' clock position by the areola [Figure - 2]. The perforated portion of drainage tube was shortened to fit in the abscess cavity [Figure - 3]. The drain was fixed to the skin with 2/0 silk suture and suction applied [Figure - 4]. A silk stitch was applied to the trochar entry wound. A sample of pus was sent for culture and sensitivity test. The patient was rested in the Out Patients Department for 1 hour and sent home on an oral antibiotic (a combination of amoxicillin and clavulonic acid in the dose of 625 mg BID for 5 days) and analgesic (Ibuprofen 400 mg QID on the first day and SOS there after). Patient was encouraged to breast-feed the baby. She was seen again on 3rd and 5th day. When the pus discharge diminished to less than 10 mL the drain was removed. The patients continued to breast feed their babies with a gap of one day. Further examinations were made after 4 and 8 weeks. Results This method of treatment has been applied to 30 patients from January 1999 to January 2005. There was no drain dislodgement in any patient. No drain replacement was required till it was removed. A sample of pus was sent for culture and sensitivity in each patient. The result was reported as sterile in eight patients and Staphylococcus aureus in 16 patients. The specimen culture report was lost in six patients. The anaerobic pus culture was not done. The bug was found sensitive to augmentin and flucloxacillin. Patients were followed up to 2 months. The drain was removed in majority of our patients on the 5th day, otherwise further visits to the hospital were required on 7th or 8th day. Another follow up was planned after 4 and 8 weeks of the procedure. The mean drainage time was 4.5 days (range: 3-8 days). The patients required convincing to continue feeding and 19 patients did continue feeding as before. However, in the rest 11 patients the affected breast was less used for feeding but the relative frequency was not recorded. So far the procedure has successfully helped in complete healing of the PBA without any complication to any patient. No recurrence of abscess or formation of fistula or sinus was noted in any patient. There was no scarring, chronic induration, or distortion of breast parenchyma. Discussion According to Haagensen, 'Abscess should be adequately drained under general anesthesia. A curved incision in the skin line is used. Penrose drain is left in place for 72 hours.'[1] The gold standard of puerperal breast abscess drainage thus described by Haagensen is supported by Webster with the addition of gauze packing.[2] Patient requires hospitalization, breast-feeding is discontinued and lactation suppressed with bromocriptine 2.5 mg twice daily for 14 days. Alternatively more potent single dose of cabergolamine is used to suppress lactation.[2] Breast distortion due to scarring or persistent discharging sinus develops in some patients.[4] Modification of this method by I and D, curettage and primary closure of the abscess cavity gives better scar formation and reduction in the cost of treatment.[5],[6] By the method of primary closure the abscess heals in 5-7 days with a failure rate of 6%.[7] By placing the incision of drainage on the infra-mammary fold of the breast scarring on the visible part of the breast can be avoided.[8] Ultrasound guided aspiration of pus, antibiotic therapy and repeated US guided aspiration of residual loculi of pus underline the importance of US imaging in modern management of PBA. Altogether 63 papers have been reported using this search.[9] It is an outpatient procedure in 53%, scar-less in 100%, complete healing occurs in 95% and breast-feeding is not interrupted in 42%.[3] A recent study concluded that breast abscesses smaller than 5 cm in diameter on physical examination can be treated effectively with repeated aspirations with good cosmetic results. Incision and drainage should be reserved for use in patients with larger abscesses.[10] In a cohort of 53 puerperal breast abscess reported by O'Hara et al. , eight were treated by primary I and D, in five patients abscess discharged spontaneously and in 18 abscesses resolved without any intervention.[11] In 22 patients breast abscess was aspirated on US guidance, in 19 abscess healed and for three patients I and D was required. Garg et al. reported a success rate of 84% in 25 patients of PBA.[12] Use of wide bore (18-gauge) needle for aspiration avoids the need for repeated puncture for aspiration.[13] Ultrasonically guided percutaneous catheter drainage of 12 breast abscesses including one PBA was found successful in all the patients.[14] Some used US guided percutaneous placement of catheter in non-puerperal breast abscess with successful healing of all the abscesses.[15] Avoidance of repeated aspirations was the advantage of US guided placement of catheter in the abscess cavity. Local instillation of antibiotics into the breast abscess cavity is probably beneficial.[16] The advantages of the present method of percutaneous suction drainage of breast abscess are many folds:
The patients easily carry out post catheter placement care of the treated breast and suction drain. Presence of the general practitioner and community nurse will make the management easier. However, this method is applicable only in drainage of large fluctuant PBA. The point of entry and exit of the suction drain trochar has to vary according to the position of the PBA in the breast. Conclusion Percutaneous placement of suction drainage catheter in PBA for 3-7 days is effective, devoid of any complication, scarless, and preserves the function of breast-feeding.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06097f4.jpg] [is06097f2.jpg] [is06097f3.jpg] [is06097f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}