 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
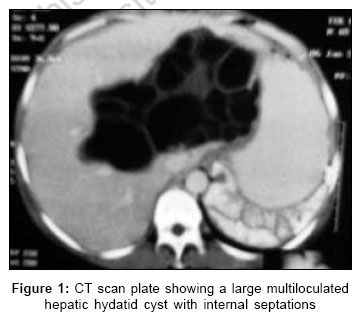
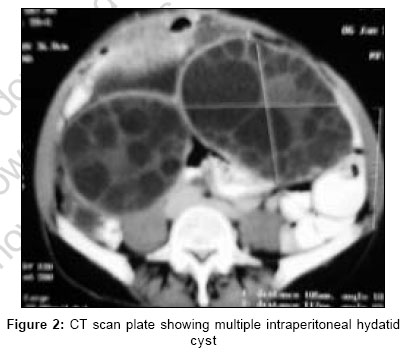
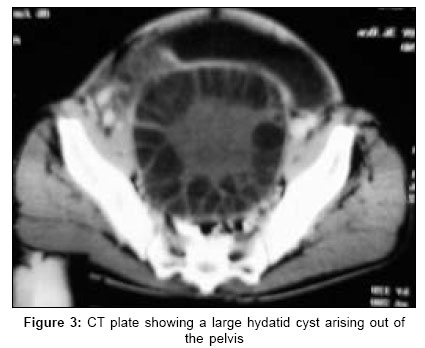
Indian Journal of Surgery, Vol. 68, No. 6, November-December, 2006, pp. 334-335 Images in Surgery Secondary echinococcosis Sahu ShantanuKumar, Singh Parvesh, Sachan PK, Bahl DigVijai Department of General Surgery, Himalayan Institute of Medical Sciences, Dehradun, Uttaranchal Code Number: is06098 A 40-year male presented with a progressive swelling in the right hypochondrium and jaundice since three months. He was operated for hepatic hydatid disease 14 years ago. Examination revealed a huge cystic mass in the right hypochondrium extending up to the umbilicus and another cystic mass in the right iliac fossa. Investigation showed serum bilirubin -2.6 mg/dl and alkaline phosphatase- 643 IU/L. Contrast-enhanced computed tomography abdomen showed a hepatic hydatid cyst and multiple disseminated intraperitoneal hydatid disease [Figure - 1][Figure - 2][Figure - 3]. Exploratory laparotomy revealed a single hepatic hydatid cyst in the right lobe and multiple disseminated intraperitoneal hydatid disease of varying sizes. Cystectomy or deroofing wherever indicated, was done for the larger cysts followed by a rigorous peritoneal lavage and multiple peritoneal drain placement. Postoperatively the patient was administered albendazole. Echinococcosis, caused by echinococcosis granulosis, commonly affects liver. Primary peritoneal hydatid disease is rare.[1] In 10-12% of cases of hydatid disease, traumatic or surgical intraperitoneal rupture of hepatic or splenic cysts results in release of brood's capsule, scolices and daughter cysts which implant and develop independently leading to multiple disseminated intraperitoneal hydatid disease or Secondary echinococcosis, the cycle taking several years.[2] Double-contrast computed tomography scan is 90-100% accurate in diagnosing secondary echinococcosis.[3] Surgery is the mainstay of treatment of secondary echinococcosis with Albendazole as the main stay adjuvant therapeutic agent.[4],[5] However the recurrence rate is very high as it is impossible to identify small residual seedlings.[2] References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06098f2.jpg] [is06098f1.jpg] [is06098f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}