 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
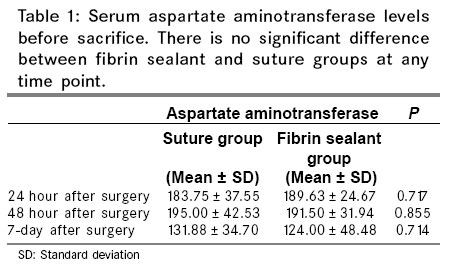
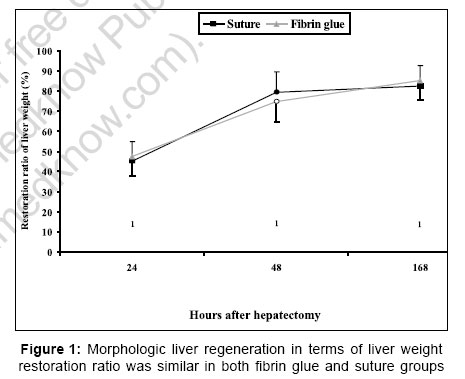
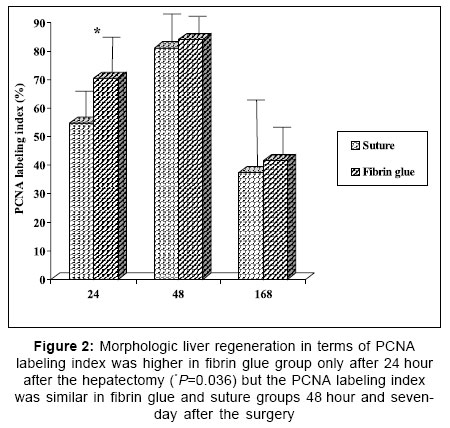
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 4-8 Original Article Does fibrin glue affect liver regeneration? an experimental study in rats Genc H, Haciyanli M, Gur S, Kamer E, Yardimci I, Tavusbay C, Lebe B, Sagol O Ataturk Training and Research Hospital, Second Surgery Clinic Code Number: is07002 Abstract Background: Fibrin glue has been used to prevent bleeding from the raw liver surface after hepatectomy. Fibrin glue has been proposed to induce hepatic regeneration but has not been clarified yet. Keywords: Fibrin, liver, regeneration INTRODUCTION Fibrin glue have been used as hemostatic and adhesive surgical adjuncts in various fields of surgery including cardiovascular surgery, general surgery, plastic and reconstructive surgery, urologic surgery and dental surgery.[1] These products are very effective in the control of bleeding in elective liver resections or in complex liver trauma.[2],[3] These products also help to reduce the postoperative biliary leak from the raw liver surface after the hepatic resections.[4],[5] Fibrin glue can also be used for the obliteration of the cystic cavity after the hydatid cyst operations.[6] Beside all those known beneficial hemostatic and adhesive role, the effect of fibrin glue on liver regeneration has not been clarified yet; although some investigators proposed that fibrin glue may have a promoting role in the repair of injured liver.[7] It may be reasonable because thrombin, the major component of fibrin glue, play the initial role in the activation of hepatocyte growth factor activator (HGFA) zymogene.[8] In this study, we developed a model in which a raw liver surface was obtained after 2/3 hepatectomy in rat, similar to that of human liver resections and investigated the effect of fibrin glue applied to that surface on regeneration of liver. MATERIALS AND METHODS About 56 males Wistar rats (160-190 g) were used in the study. Rats were kept under constant environmental conditions with a 12 hour dark and light cycle and fed freely with water and normal laboratory chow. The animals received human care in compliance with the guidelines of Duke University Institutional Animal Care and Use. The local ethic committee of the Hospital approved the study. The surgical procedures were performed under semisterile conditions at the same time of the day to avoid circadian variations. Rats were anesthetized by intra-peritoneal injection of ketamine hydrochloride 100 mg/kg (Eczacibasi, Istanbul) and xylazine 20 mg/kg (Deva, Istanbul). Midline incisions were used for the procedures. Partial (70%) hepatectomy was performed according to the method of Higgins and Anderson.[9] A standardized triangle of 1 cm each side, at the free edge of remnant lobe was resected and a standard raw liver surface was obtained. The rats were randomized to two groups: Hepatic raw surface was repaired with a horizontal matress suture of 6/0 polyprolene (Ethicon, Johnson &Johnson, USA) in group one and resected liver surfaces was sealed by fibrin glue (Beriplast® P Kombi-set, 1 mL, Aventis Behring) in group two. The liver cut surfaces were held together with a gentle pressure for the time necessary to stop bleeding and to join the surfaces. The model was validated in a pilot study. Post-operatively animals had free access to water and food. Four animals from each group were immediately sacrificed and the resected lobes and triangles and remaining lobes were weighed to find the percent of resected lobes and triangles over total liver weight (TLW). The resected lobes constituted the 67.7% (±2,2) of TLW in suture group and 68% (±3.1) of TLW in fibrin glue group. The resected triangle comprised 3.8% (±0.3) of TLW in suture group and 3.3 ± 0.4% of TLW in fibrin glue group. Overall, two-third hepatectomy was 68.11% (±1.35) of total liver weight and the triangle was 3.51% (±0.44) of TLW in first eight rats. The mean resected liver mass constituted 71.6% (±1.6) of TLW. Then we accepted this value for further calculations. Rats from each group were humanly killed by thiopenthal (IE Ulagay, Istanbul) overdose at 24, 48 hours and seven day after the surgery. Blood samples were obtained from inferior vena cava after the resection and before the sacrifice. Remnant liver was resected, weighed; a gram of liver tissue near the raw surface was cut and soaked in 10% formaldehyde solution. Assessment of cell injury The degree of hepatic injury was assessed using serum levels of aspartate aminotransferase (AST), which is an established marker of hepatocellular injury in rats.[10] AST serum levels were measured using standard laboratory methods. Assessment of morphologic liver regeneration Morphologic liver regeneration was evaluated in terms of the restitution of the liver weight that was determined as the percentage of regenerated liver mass per total liver mass and using proliferating cell nuclear antigen (PCNA) labeling index. The liver restoration ratio was calculated. In brief, the excised liver was on average 71.6% of TLW so TLW was estimated assuming 71.6% excision. The liver restoration ratio was expressed as a percentage of the restored liver weight per total liver weight. Liver samples were immunostained for PCNA. Immunohistochemical procedure About 5μ sections from each paraffin block were taken to poly-L lysine coated slides for immunuhistochemical staining. Standard streptavidin biotin immunperoxidase method was used for immunostaining with PCNA (DAKO, M0879, dilution: 1/100) antibody. The tissue sections were deparaffinized in xylene, rehydrated in alcohol series, immersed in distillate water. The sections were then boiled in citrate buffer solution (10 mmol/L, PH: 6.0) in a microwave oven, three times for 10 minutes for epitope retrieval. Endogenous peroxides activity was blocked using a 0.3% solution of hydrogen peroxide in phosphate buffered saline (PBS) at room temperature for 10 minutes and rinsed with TRIS buffer. Primary antibodies were applied for 30 minutes at room temperature and washed in TRIS buffer. Linking antibody and streptavidin peroxidase complex (Dako LSAB Kit, K = 675; Carpinteria, USA) were added consecutively for ten minutes at room temperature and washed in TRIS buffer. Peroxidase activity was visualized with 0.03% 3,3-diaminobenzidine tetrahydrochloride (DAB) (Sigma Chemical Co, St. Louis, Missouri, USA), applied for 5 minutes. The sections were then washed in deionized water, counterstained with Mayer's Hematoxylin and mounted. Appropriate tissue section known to react with PCNA was used as positive control. Evaluation of the staining For each case, nuclear PCNA expression of the hepatocytes was evaluated in a light microscope and expressed as the percentage of stained nuclei by counting 1000 hepatocytes in high power fields. All slides were evaluated in blinded fashion by one of the authors. Statistical analysis The data were expressed as the mean ± standard deviation (SD) and analyzed with the SPSS (10.0 for Windows) statistics package. Student t -test was used for quantitative variables to examine the significance of differences with a P value less than 0.05 as the minimum level of significance. RESULTS No mortality was detected in groups. Fibrin sealant and suture both achieved effective hemostasis in seconds. The mean serum AST levels at 24, 48 hour and seven day after the surgery are shown in [Table - 1]. The AST levels were high in both groups 24 hours and 48 hours after the surgery and the difference between groups were not significant ( P =0.717 and P =0.855, respectively). At day seven, although the mean serum AST levels were decreased in both, suture and fibrin sealant groups, they were still above the normal limits and there was no difference between the mean AST levels of the groups ( P =0.714). So the same level of injury was obtained in groups. The liver restoration ratio, expressed as the percentage of regenerated liver mass per total liver mass was similar between two groups and there was no differences between the groups at each studied time point [Figure - 1]: The percent of the restored liver weight in suture and fibrin groups were 45% (±17.79) and 47.63% (±11.38) at 24 hour ( P =0.730); 79.50% (±16.21) and 74.75% (±10.51) at 48 hour ( P =0.415); 82.5% (±16.21) and 85.38% (±9.68) at day seven ( P =0.673). The PCNA labeling index after the partial hepatectomy in both groups increased at 24 hour (54.62 ± 11.02% in suture group vs. 70.38 ± 15.70% in fibrin group) reached a peak at 48 hour (81.00 ± 10.74% in suture group vs. 84.00 ± 7.19% in fibrin group) and decreased at seventh day after the surgery (37.38 ± 24.49% in suture group vs. 41.63 ± 10.46% in fibrin group) [Figure - 2]. The PCNA labeling index was higher in fibrin glue group 24 hour after the surgery ( P =0.036) but there was no difference between the groups at 48 hour ( P =0.522) and seven day ( P =0.662) after the surgery. DISCUSSION Post-hepatectomy hepatic insufficiency is one of the major problems associated with the liver surgery. Although post-hepatectomy liver insufficiency is a more serious problem in the cirrhotic liver, it also constitutes a major problem in normal liver tissue. Regeneration and restoration of the liver mass after partial hepatectomy in healthy rats has been extensively investigated and recently attempts have been directed to increase or improve the liver regeneration after hepatic resections.[11],[12] But the effect of fibrin glue on this regeneration has not been clarified yet probably because of a difficulty in developing a hepatectomy model that enables the application of fibrin glue. Partial hepatectomy is a good model of compensatory cellular growth. We further removed a standardized triangle from the remaining lobe hence a raw liver surface was obtained. So fibrin glue can be applied to that surface which is similar to the application of fibrin glue on the raw surface of liver in human liver surgery. In pilot study, we observed that 2/3 hepatectomy constituted almost 68% of TLW and this triangle constituted almost 3.5% of TLW. Total resected liver tissue was almost 71.6% of TLW and it was accepted as reference value for further calculations. Previously, Tovar et al . reported such a standardized triangle resection of liver for hemostasis study but it was not a partial hepatectomy model.[7] Fibrin glue has been extensively used for hemostasis in liver surgery during the last decade. Both suture and fibrin glue effectively controlled bleeding in seconds in our study. Since the raw liver surface became very small after the suture process, so we didn't apply fibrin glue to the raw surface after suturing. Liver regeneration is a complex phenomenon that involves the activation of adult hepatocytes and possibly of liver precursor cells. After partial hepatectomy or toxic liver injury, the regeneration is regulated by a variety of molecular signals such as cytokines and growth factors. Hepotocyte growth factor (HGF) is the most potent stimulus for hepatocyte growth and DNA synthesis and this process is essential for hepatocyte proliferation during regeneration.[13],[14] It stimulates DNA synthesis of hepatocytes in toxically or mechanically injured liver tissue or during liver infection. HGF is secreted as an inactive form and activation is initialized in the injured liver by a protease named HGF activator (HGFA).[15],[16] HGFA itself is first synthesized as an active precursor and then activated by proteolytic process in response to liver injury and thrombin has been proved to play the initial role in activating the HGFA zymogene.[8] The major component of the fibrin glue is thrombin. Schamandra et al . showed that fibrin glue occlusion of the hepatobiliary tract induces the therapeutic and prophylactic effects on chronic toxic liver damage by activation of the HGFA/HGF process: Fibrin glue was injected into the proximal biliary tree in a toxic injury model and enhances hepatocyte regeneration.[13] In terms of both restoration ratio and PCNA labeling index, fibrin glue did not increase morphologic liver regeneration in this study. But, previously, Tovar et al. showed that regeneration was faster in the fibrin sealant group than suture and hot coagulation group and attributed this increase probably to supporting role of fibrin glue in wound healing.[7] Disappearance of necrosis and perilesional fibrovascular tracts at 40 days post-operatively was the only parameters that leaded researchers to conclude a faster regeneration but assessment of liver regeneration should be done using more objective criteria such as the liver restoration ratio and the PCNA labeling index. In our study regeneration was investigated in a healthy liver tissue and in a hepatectomy model not in a toxic injury model. The effect of fibrin glue on hepatocyte regeneration in cirrhotic liver should be assessed in another study using this experimental model. CONCLUSION As a result, our study is unique in creating a raw surface similar to that of liver resections in human and a more identical model for the application of fibrin glue to human liver resections. The fibrin glue applied to the raw liver surface controlled bleeding effectively but it did not enhance liver regeneration after 70% hepatectomy in rats. References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07002f1.jpg] [is07002t1.jpg] [is07002f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}