 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
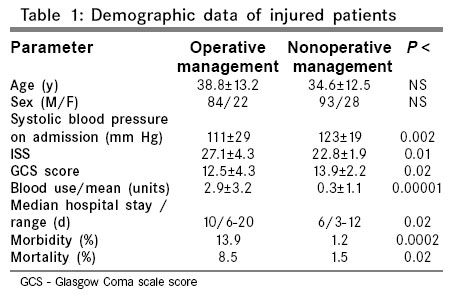
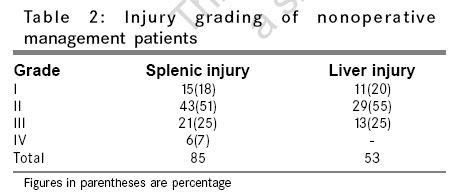
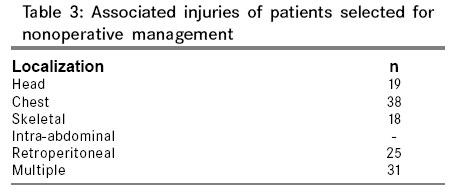
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 9-13 Original Article Nonoperative management of blunt splenic and liver injuries in adult polytrauma Kirshtein Boris, Roy-Shapira Aviel, Lantsberg Leonid, Laufer Lie, Shaked Gad, Mizrahi Solly Department of Surgery A, Soroka Medical Center, Faculty of Health Sciences Ben Gurion University of the Negev, Beer Sheva Code Number: is07003 Abstract Background: Isolated splenic or hepatic injuries are present in approximately 30% of all cases of adult abdominal trauma. Most authors quoted above have limited nonoperative management (NOM) to patients with isolated organ injury. Results of NOM following blunt hepatic and splenic trauma in patients with multiple injuries were evaluated in this study.Materials and Methods: Retrospective chart review was performed on multiple injured adults with splenic and liver injures resulting from blunt trauma. Associated injuries, clinical signs at presentation, used diagnostic tools, injury grading, transfusion requirements, morbidity and mortality were documented. Results: Medical records of 275 patients aged from 17 to 81 years with blunt splenic and liver trauma and associated injuries were analyzed. Patients with hemodynamic instability or obvious peritoneal signs were excluded from further study. Surgery was indicated in 106 patients without response or transient response for fluid challenge. 131 of 237(55%) patients were selected for NOM: 78 with splenic, 46 with liver and 7 with injuries to both. 25(19%) patients were older 55 years. The mean injury severity score was 25.2. Injury grade ranged from I-IV and the degree of hemoperitoneum was from mild to severe. 8 patients failed NOM (6%). Mean blood transfusion requirement during first 24 hours at admission was 0.3 units. Morbidity rate was 1.2%. Two patients (1.5%) died following severe head trauma. Conclusion: Nonoperative strategy is the preferred modality for the care of blunt splenic and liver injuries in the hemodynamically stable patients, irrespective of age, grade of injury, associated injuries or degree of hemoperitoneum. Keywords: Blunt abdominal trauma, nonoperative management, spleen and liver injury Introduction Isolated splenic or hepatic injuries are present in approximately 30% of all cases of adult abdominal trauma.[1],[2] In recent years, following the initial success of Upadhyaya and Simpson with nonoperative management (NOM) of splenic injuries in children,[3] more and more stable patients with blunt splenic injuries are treated nonoperatively with reported success rates of 14-100%.[4],[5],[6],[7],[8],[9] Recent studies documented successful extension of this approach to the care of hepatic, renal, pancreatic and multiple injuries.[10],[11],[12],[13],[14],[15] Increasing use of high quality computed tomographic imaging and its interpretation leads to redefinition of the criteria for NOM of splenic and hepatic injuries.[16],[17],[18] Most authors quoted above have limited NOM to patients with isolated organ injury. In this paper, we present our experience with NOM of hepatic and splenic injuries in patients with additional extra- and intra-abdominal injuries. Materials and Methods In this retrospective chart review, medical records of 275 consecutive adult patients (age over 16 years) with blunt splenic and liver injuries admitted to Soroka University Hospital Level I trauma center in South Israel between 1991 and 2005 were analyzed. The patients were identified from Hospital Medical Records Service by ICD codes (864.00, 864.01, 864.05, 864.11, 864.15; 865.00-865.03, 855.11, 865.12) and trauma unit registry. The following variables were recorded: age, gender, mechanism of injury, initial Glasgow Coma Scale score (GCS) and systolic blood pressure, associated injuries, injury severity score (ISS), diagnostic procedures, injury grade, number of units of packed blood cells transfused within the first 24 hours at admission, morbidity and mortality rate. The diagnosis of hemoperitoneum was confirmed by abdominal ultrasonography, computerized tomography (CT)-scan or by peritoneal lavage (DPL). From 1996, focused abdominal sonography trauma (FAST) has largely replaced DPL in the initial assessment of the blunt trauma victim. Solid organ injuries were classified by using the Organ Injury Scale Committee of the American Association for the Surgery of Trauma standards according the results of abdominal CT-scan and ISS. Hemodynamically unstable patients and patients with obvious peritoneal signs underwent immediate abdominal exploration and were excluded from further analysis. The signs of hemodynamic instability included: arterial hypotension (systolic pressure lower than 100 mmHg) and/or tachycardia at admission (pulse more than 100 beats per minute). Absence of response or transient response to fluid challenge (1000-2000 ml Ringer's lactate) was indication to operative treatment. Victims without tachycardia and/or hypotension at admission were concluded as hemodynamically stable. Patients responded to fluid challenge with decreasing in pulse rate and increasing of blood pressure was included in category of stable and was treated nonoperatively. Patients selected for observation were admitted to the intensive care unit for 24-48 hours for continuous serial physical examination, vital signs and serial hematocrit measurement. All patients were examined by surgeon on call (usually senior resident) every hour or in case of hemodynamic changes. With increasing experience of trauma team in NOM treatment during the last 3 years we decrease a patients bed stay from one week to 3 days. Up to year 1999 a follow-up CT scan was obtained at 72 hours and 10-14 days after admission. The amount of hemoperitoneum was measured as described by Levine et al .[17] An attending radiologist and an attending surgeon interpreted all imaging studies. Later CT scan did not affect discharge as it was performed in outpatient department. Since 1999 we changed our radiological follow-up policy and routine CT scan was performed in complicated or clinically needed cases only. Data was entered into computer database program and statistical comparisons between the NOM and OM groups were performed with EpiInfo Version 6.04a (Center for Disease Control, Atlanta, GA, US). Tests for statistical significance included the Chi-square and Fisher's exact tests. A P < 0.05 was considered significant. Results There were 201 men and 74 women with age range from 17 to 81 years old (mean 38.2 years). 35 patients (13%) were older 55 years. Mechanism of injury was motor vehicle accident in 215(78%) of cases, fall from height in 36(13%), assault in 23(8%) and blast in 1(0.4%). 29 hemodynamically unstable and 9 patients with obvious peritoneal signs were taken immediately to the operating room for exploratory laparotomy and were excluded from further analysis.149 of 237(63%) remaining patients sustained injury to spleen, 61(26%) to liver and 27(11%) to both. GCS score at admission was from 3 to 8 in 39, from 9 to 12 in 19 and from 13 to 15 in 179 patients. Transient response or absence of response to fluid challenge was indication for surgery in 106 patients. Overall 131(55%) patients were selected for NOM. Patients characteristics are summarized in [Table - 1]. Age and sex distribution were similar in the two groups, but the NOM patients had a higher GCS score and systolic blood pressure on arrival than the operated group. 78 of 131(60%) patients in NOM group has injured spleen, 46(35%) - liver trauma and 7(5%) - combined trauma of both. These included 25 of 35(71%) patients older 55 years old. CT grading of splenic and liver injuries is presented in [Table - 2]. 6 patients had grade IV splenic injury with flushing of contrast dye on abdominal CT-scan. Assessment of degree of hemoperitoneum on CT-scan revealed small amount of intraabdominal blood in 29, moderate in 41 and severe in 61. Additional associated injuries are listed in [Table - 3]. Injury grading in operating patients was unavailable. Mean transfusion requirement during first 24 hours of admission was 0.3 blood units (range 0-2). Overall 26(20%) patients in NOM group and 94 (89%) in OM group were transfused. In NOM group patients required blood included those with higher injury grade and additional pelvic and long bone fractures. One NOM patient developed an infected intra-hepatic bile collection, which resolved after percutaneous drainage. Two other patients in this group with admission GCS score 3, remained comatose and died later from complications of head injury. All other patients did well. NOM patients had shorter hospital stay. There was no difference in hospital stay after changing CT follow-up policy. Overall morbidity and mortality rate in NOM patients was 1.2% and 1.5% respectively. NOM failed in 8(6%) patients. Decreasing hematocrit and requiring more than 4 blood units during the first 24 hours from admission was indication for laparotomy in 4 patients. Delayed diagnosis of diaphragmatic injury in one and pancreatic transection in another case was revealed in second abdominal CT scan performed 24 hours after admission. CT was performed on the morning after clinical suspicion and films revision. Small tear of left diaphragm without dislocation of intraadbominal organs and splenic laceration were found on surgery in first patient. This patient required splenectomy during abdominal exploration and suturing of diaphragm. Distal pancreatectomy and splenectomy was performed in second case. One poor compliance drug abuser underwent splenectomy 48 hours after admission despite hemodynamic stability. Hypovolemic shock at readmission 2 weeks after injury in patient with known grade II splenic injury was indication to splenectomy in other case. A small amount of hemoperitoneum with a healing nonbleeding splenic tear was found during laparotomy. The cause of his worsening was large hemothorax that was treated by thoracal drainage. He was discharged uneventfully after 9 days. Discussion In 1893, Reigner[19] described the first successful splenectomy for blunt trauma. Senn,[20] in 1903, described nonoperative management of splenic injury. Kocher who reported a NOM mortality rate of about 90%,[21] quickly challenged him. Since Kocher's report, splenectomy became the standard of care for the injured spleen. In 1968, however, due to concerns with overwhelming post splenectomy sepsis, the Hospital for Sick Children in Toronto published its successful experience of nonsurgical approach to pediatric splenic injuries.[3] From 1980's numerous investigators reported variable success rates ranging from 14 to 100% in the NOM of blunt splenic injuries in adults.[4],[5],[6],[7],[8],[9] Complex splenic injuries, preexisting splenic pathologic conditions, older age, blood transfusion requirement or neurologic injuries are not universally accepted as reasons to avoid NOM, as was mandated in early reports.[22],[23],[24],[25] Success in NOM of splenic injuries and high complication rate in liver trauma surgery led to it application for patients with hepatic trauma. NOM of liver injury has now evolved into a common practice, following reports revealing success in 85 to 100% of patients.[12],[14],[15],[16],[26],[27] Immediately available hospital facilities including intensive care unit and 24-hours emergency operating room are important resources for success in NOM of patients with blunt abdominal trauma. In our series we found 52% of multiple traumatized patients with blunt splenic, 75% with liver and 26% with combined spleen and liver injuries were successfully managed nonoperatively, which is consistent with reports from previous studies. Most studies of NOM have excluded patients with extra-abdominal conditions particularly neurologically impaired patients. A recent review of blunt splenic injuries suggested that candidates for nonoperative treatment "must have suffered an isolated splenic injury in minimally injured patients".[7] In contrast, both Archer[10] in adults and Coburn[13] in children and adolescents did not find increased morbidity or failure rate in the multiply injured patients with NOM. The rationale for excluding neurologically impaired patients was the inability to perform reliable physical examination. However, the reason for converting NOM to OM in these studies was either falling hematocrit or hemodynamic deterioration. Alteration in the physical examination played a little role in the decision makes process. Repeating bedside abdominal sonography or CT scan is not playing a significant role in such cases. We have selected early to extend NOM to selected stable patients with associated injuries that not require an abdominal operation. 19 patients in this group had severe head injury, other 111 had associated multiple injuries and even 2 patients had traumatic thoracic aortic rupture. One of them underwent thoracotomy and patching of aortic tear. Aortic stent was inserted in the second case. Their grade II liver injuries were treated conservatively. Overall, of our 131 NOM patients, 123 were uneventfully discharged without an abdominal operation, in spite of having associated injuries. Interestingly, all the patients who had DPL as the primary diagnostic tool were operated upon. The use of FAST, in the hands of the surgeon, is just as accurate for the detection of hemoperitoneum.[28],[29] Its adoption in our emergency trauma room in 1996 has increased the number of patients with blunt splenic and liver injuries treated without surgery up to 79%. Any abnormality present on ultrasound in stable patients was confirmed with abdominal CT scan to determine specific organs injured and potential for NOM. CT should be used preferentially over DPL and US to increase overall splenic and hepatic salvage.[4] Data obtained from CT scan included grade of injury, quantity of hemoperitoneum, presence of arterial extravasation and concomitant abdominal injuries. Diagnosis of active bleeding per CT requires performing an angiographic embolization of bleeding source when possible.[30] However, 6 patients with grade IV splenic injuries and flushing of contrast dye on CT scan underwent successful NOM without additional intervention. Stable hemodynamics and hemoglobin level, close monitoring, controlled hypotension were factors of success. Routine pre- or post discharge CT scans have been frequently ordered to document healed splenic or liver injuries and aid in determining a time frame for the patient to return to full activity. Recent reports[31],[32] suggest that post discharge activity limits for spleen and liver injuries managed by NOM should not exceed those after laparotomy. Therefore, it would appear that routine pre- or post discharge CT scan is unnecessary to guide activity restrictions if the patient remains asymptomatic. From 1999 we stop routine abdominal CT scan performance before discharge of patients without abdominal symptoms. The need for blood products in treatment of splenic and liver injuries had led to further questions and controversy because risk of transfusion diseases.[33] Luna and Dellinger[34] suggested that the risk of death due to blood transfusion in successful NOM of splenic injury exceed that of immediate operation of injured spleen. Two blood units in isolated spleen injury limit spleen NOM. Nonoperative treatment may be continued in patients with higher transfusion requirements only if could be establish that these additional transfusions were necessitated by associated injuries. Our data in multiple trauma patients consistent with other recent reports in literature[10],[11] and demonstrate significantly lower transfusion rate in NOM patients. Some authors[10] in 1990-s argued age over 55 years prohibit NOM in splenic or hepatic injuries. However, the data support this argument leave a lot to be desired. With growing experience of NOM in elderly patients different reports[35],[36] conclude that age should not be a criteria for NOM of blunt splenic injuries. Older patients with high-grade injuries and pelvic free fluid are greater risk for NOM failure. Patients with these findings must be monitored closely. Failure of NOM in this population is associated with increased morbidity and mortality.[36] Careful selection of patients older 55 years must be made to minimize morbidity and mortality from failed attempts. At any event, the 25 patients older 55 selected for NOM in the present series were managed successfully. Currently, the reported failure rates for NOM ranges from 15-25%.[4],[5],[6],[7],[8],[9],[12],[14],[26],[27] In this series, the failure rate was 6%. This is a result of patient's selection, which is evident by the significantly higher GCS and systolic blood pressure at admission in NOM group. In addition, there were 11(10%) non-therapeutic laparotomies in the OM group. This fact indicates that not all patients who could have been managed nonoperatively were right selected. This is a field for more experience in management of blunt splenic and liver injuries. The use of laparoscopic splenectomy or splenic preservation in stable patients with delayed splenic rupture or NOM failure may be inspecting in future. Conclusion We conclude that NOM is safe and effective in selected stable patients with splenic and liver injuries. It appears that neither age, injury grade, perceived amount of intraperitoneal blood, nor associated injuries, are contra-indications to NOM. The most important selection criterion is hemodynamic stability. The indication for conversion from NOM to OM is based on additional injuries detected by subsequent imaging and on hemodynamic criteria, not on physical examination only. References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07003t1.jpg] [is07003t3.jpg] [is07003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}