 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
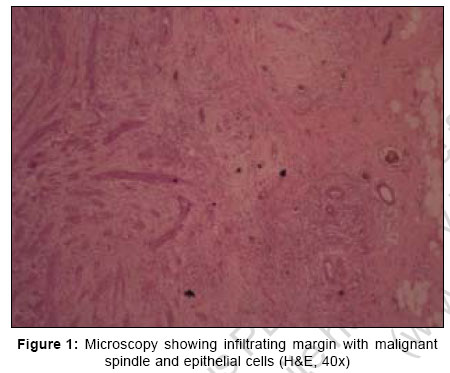
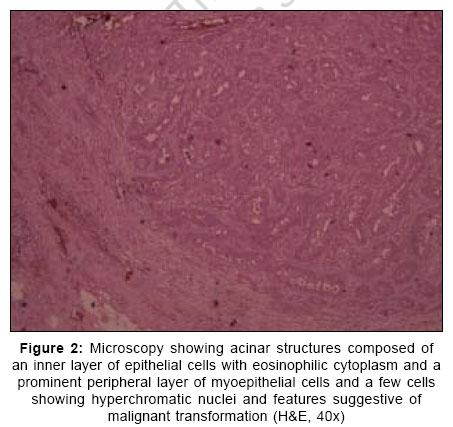
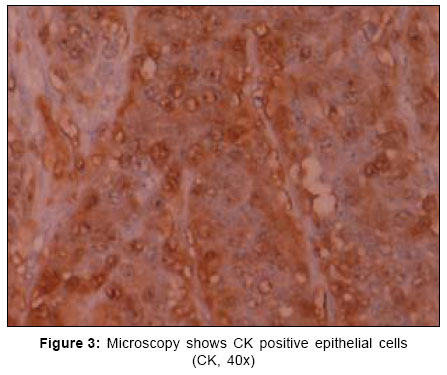
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 14-16 Case Report Malignant adenomyoepithelioma of the breast Suresh Attili VS, Saini Kamal, Lakshmaiah KC, Batra Ullas, Malathi M, Ramachandra C Department of Medical Oncology, Kidwai Memorial Institute of Oncology, Bangalore Code Number: is07004 Abstract Malignant adenomyoepithelioma of the breast is a rare tumor characterized by biphasic proliferation of both epithelial and myothelial cells. Here we report a 20-year-old female presented to us with recurrence of a breast lump shortly following lumpectomy. Histopathological examination suggested malignant adenomyoepithelioma. She had undergone modified radical mastectomy, received local radiation to the chest wall and six courses of adriamycin and cyclophosphamide. She remains in complete remission at 18 months follow-up. The present case is rare in several respects. The age of presentation was 20 years, much less than what has been reported. Mammography showed micro-calcifications, thus far not described. In addition, our patient had an exceptionally aggressive tumor that recurred within two months of lumpectomy. This tumor also showed good chemo sensitivity.Keywords: Breast, malignant adenomyoepithelioma, mammography, recurrent Introduction Adenomyoepithelioma of the breast, first described by Hamperl in 1970, is a rare tumor characterized by biphasic proliferation of both epithelial and myothelial cells.[1] These tumors are usually benign. Malignancy may arise through neoplastic transformation of the epithelial component or myothelial component or both.[2] By strict definition, malignant adenomyoepithelioma is one in which both cellular components undergo malignant transformation. Till 1999 only 11 cases had been reported.[2] Since then, with better awareness of this entity and characterization of histologic and immunohistochemical features, a few more cases have been reported with largest series comprising of 35 cases.[3] It is usually less aggressive, however, more aggressive forms can exist. So far, such an aggressive tumor is not reported from India (Medline). Here, we report one such case that recurred in 2 months, reviewed the literature and discussed the diagnosis, treatment, and outcome. Case Report The patient is a 20-year-old female who first noticed a lump in her right breast six months ago. She was seen at a local general hospital where she underwent lumpectomy three months ago, records and slides of which were not available. Two months after surgery, she noticed a recurrence of the lump and a gradually increasing swelling in her right axilla. After she presented to our center, workup revealed normal hematologic and biochemical parameters. Fine needle aspiration cytology from the breast lump and right axilla were positive for malignant cells. Mammography of the right breast showed an irregular mass lesion of 3x4 cm in the upper outer quadrant, with micro-calcifications suggestive of malignancy. Computerized tomography (CT) thorax, abdomen, and nuclear bone scan were all normal. ER, PR and HER2/Neu were all negative. After an inter-disciplinary meeting, it was decided to subject her to modified radical mastectomy with local radiation and six courses of anthracycline based chemotherapy. The histo-pathological specimen showed a gross lesion of 3.4x4.5 cm. Microscopy showed a histology of adenomyoepithelioma at one end i.e., epithelial acinar structures with myoepithelial cell proliferation [Figure - 1],[Figure - 2]. This lesion at the other end showed infiltrating margins, with malignant spindle cells and epithelial cells. The spindle cells were positive for the SMA and S100 and infiltrating malignant epithelial cells were positive for CK and EMA [Figure - 3]. Seven out of 20 dissected lymph nodes were positive for malignant cells. After two courses of adriamycin and cyclophosphamide, re-assessment showed a suspicious 1 cm lesion in the middle lobe of the right lung. It was decided to continue the same chemotherapy regimen. After two more cycles chest CT was normal. She was given tele-radiotherapy to the right chest wall, the dose being 45 Grey in 25 fractions. Following this, she received two more cycles of chemotherapy. The patient is in complete remission in last follow-up done 18 months post therapy. Discussion 'Malignant transformation of adenomyoepithelioma' and 'malignant adenomyoepithelioma' are two distinct entities. Malignant transformation of adenomyoepithelioma is an uncommon tumor characterized by the neoplastic proliferation of either epithelial or myothelial component of the breast. Malignant adenomyoepithelioma of the breast is a rare lesion characterized by malignant proliferation of both epithelial and myoepithelial cells. Till 1999 only 11 cases had been reported.[2] Since then, with better awareness of this entity and characterization of histologic and immunohistochemical features, a few more cases have been reported with largest series comprising of 35 cases.[3] So far it is reported in women aged 26-76 years.[1],[2],[3],[4] Clinically, it present as a palpable, non tender and centrally located mass, although atypical presentation is known to occur.[5] The natural history of biphasic malignant adenomyoepitheliomas is largely unknown with a reported follow-up of 12-64 months in the literature.[1],[2],[3],[4],[5],[6],[7],[8] The metastatic potential of this entity is not well studied. It appears to have hematogenous rather than lymphatic spread and usually occurs in primary tumors of more than 2 cm size.[1],[2],[3],[4] The evolution of malignant adenomyoepithelioma seems to begin with adenosis with or without myoepithelial hyperplasia, proceeds to benign adenomyoepithelioma and ends in a malignant tumor that still may contain residues of its precursor lesion.[2] Because of the varied and hypercellular nature of these tumors, diagnosis by cytology is difficult.[7] Core biopsy provides more accurate information. If a benign lesion is diagnosed by cytology, total excision of the lesion with a margin of uninvolved breast tissue is recommended. Malignant adenomyoepithelioma usually stains positive for SMA, smooth muscle myosin (SMM), and S-100 proteins. Based on their growth pattern, the tumor is classified as tubular, lobulated or spindle cell variants.[5] Combinations can also exist. The imaging features of malignant adenomyoepithelioma are non-specific and not well representative of the underlying pathology. Benign features (circumscribed lesions without parenchymal distortion) or features suspicious for malignancy (poorly defined lesion margins, distortion of the surrounding breast parenchyma, distal acoustic shadowing on sonography) may be seen.[8] However, no microcalcifications, as seen in the present case, have been reported so far. The best predictor for local recurrence is the surgical margin. If the excision margin is narrow or incomplete, re-excision to gain adequate margins is recommended. Tubular variants and some lobular tumors with high mitotic activity are particularly prone to local recurrence.[5] There is no evidence that the relative proportions of individual cell groups is a risk factor for local recurrence. If carcinomatous element (epithelial or myoepithelial) is present histologically in an excised adenomyoepithelioma, it should be treated as a carcinoma.[8] The present case is rare in several respects. The age of presentation was 20 years, much less than what has been reported. Mammography showed micro-calcifications, thus far not described. In addition, our patient had an exceptionally aggressive tumor that recurred within two months of lumpectomy. This tumor also showed good chemosensitivity and remains asymptomatic after 18 months of follow-up. References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07004f3.jpg] [is07004f2.jpg] [is07004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}