 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
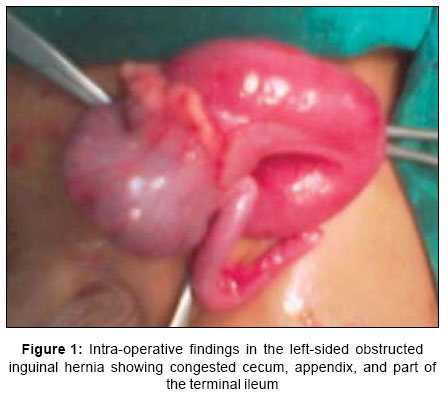
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 17-18 Case Report Left-sided incarcerated Amyand's hernia Gupta Nidhi, Vinay Wilkinson TRaju, Wilkinson Anne, Akhtar Murtaza Department of Surgery, NKP Salve Institute of Medical Sciences and Research Centre, Hingna, Nagpur Code Number: is07005 Abstract Amyand's hernia refers to the presence of the appendix within the hernial sac. Though it was first described 270 years ago in an 11 years old boy, it remains relatively unknown because of the rarity of its occurrence. It usually occurs on the right side. We are reporting a very rare case of left sided incarcerated Amyand's hernia in an 11-month-old boy.Keywords: Amyand's hernia, appendix, congenital inguinal hernia, incarcerated hernia INTRODUCTION Claudius Amyand (1680-1740), a Sergeant surgeon to King George, reported the first successful appendicectomy in an 11 years old boy, in whom a perforated appendix was found in the hernial sac. Since then, the presence of the appendix within an inguinal hernia has been referred to as 'Amyand's hernia' and still remains a rare occurrence.[1],[2] We are reporting a very rare case of left-sided incarcerated congenital inguinal hernia, with the appendix and caecum as contents, in an 11 month- old boy. CASE REPORT An 11-month-old boy presented as an emergency, with a tender non-reducible left inguinal hernia, bilious vomiting, abdominal distention, and oliguria since the past 36 hours. The child had been seen previously in the OPD for umbilical hernia and congenital inguinal hernia and had been advised surgery. Presently on examination there was a tender, irreducible swelling in the left inguino- scrotal region. The peripheral pulses were feeble and the anterior fontanel was depressed. The umbilical hernia had resolved and the cicatrix did not show any defect. A provisional diagnosis of left obstructed inguinal hernia with mild dehydration was made. After initial resuscitation and administration of intravenous antibiotics he was given general anesthesia with a caudal block. A transverse incision was made above the pubic tubercle and after opening the Scarpa's fascia the hernial sac was identified. After opening and aspirating out the fluids an engorged appendix along with the cecum and loaded terminal ileum was identified [Figure - 1]. There were no adhesions between the hernial sac and the contents of the hernia. Due to the engorged appearance of the appendix, it was decided to perform an appendicectomy. The inspissated fecal matter in the terminal ileum was milked into the cecum and ileo-cecal loops were replaced into the peritoneal cavity. The hernial sac was dissected all around the spermatic cord and herniotomy was carried out. The child had an uneventful post-operative period. The histopathology report of the appendix confirmed congestive changes in the appendix. Retrospectively situs inversus and malrotation was ruled out by radiography of the chest and abdomen, as well as ultrasonongraphy of the abdomen. DISCUSSION The term Amyand's hernia has been used to describe occurrence of an inflamed appendix within an inguinal hernia, a perforated appendix within an inguinal hernia or a non-inflamed appendix within an irreducible inguinal hernia. This is a rare condition found approximately in 1% of adult inguinal hernia repairs and association with appendicitis is even more rare.[2] Pre-operative diagnosis of hernial appendicitis is very difficult and when it occurs it is usually is diagnosed as strangulated inguinal hernia.[3] Pre-operative CT scan of the abdomen can reveal unsuspected diagnosis of Amyand's hernia.[4],[5] Most of the cases occur on the right side because of the normal anatomical position of appendix. In addition, right-sided inguinal herniation is more common. Left-sided Amyand's hernia can be associated with situs inversus, intestinal malrotation or mobile cecum. Appendicetomy is carried only if the appendix is inflamed. Appendicectomy and hernioplasty maybe performed at the same time without prosthesis implants due to contamination of the operating field.[2],[3],[6] Endoscopic total extraperitoneal repair of right-sided Amyand's hernia has also been reported.[7] In our case the patient was an infant, with the cause of left-sided Amyand's hernia probably being due to a mobile cecum, as the other causes of malrotation of the gut and situs inversus were ruled out radiologically. We are reporting this case for its rarity of occurrence, especially on the left side, as only isolated case reports have been reported so far. Awareness of this condition would be helpful in diagnosing this condition pre-operatively. ACKNOWLEDGEMENT We thank Dr Raman Gupta, Resident, Dept of Radiology NKPSIMS, for helping us with Ultrasound and X rays of this patient and Dr Sadhana Mahore Professor and Head Dept of Pathology NKPSIMS for the histopathology report of this patient. References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07005f1.jpg] |
| |||||||||

{kind=link}