 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
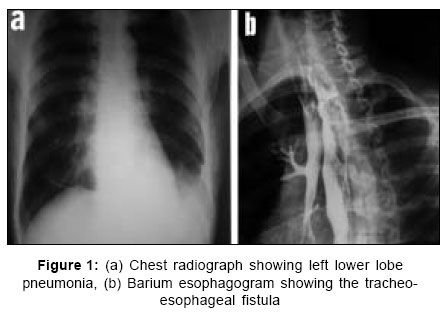
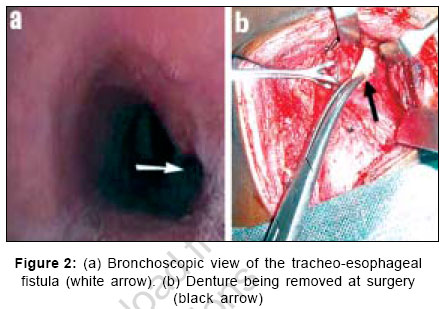
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 19-21 Case Report Acquired tracheo-esophageal fistula caused by a denture Rekha P, Sajitha M, Pappachan JM, Babu Akash, Jayakumar TK, Sukumaran P Department of Internal Medicine, Kottayam Medical College, Kerala Code Number: is07006 Abstract A majority of the cases of acquired tracheo-esophageal fistula (TEF) are a result of complication of malignancy. Acquired non-malignant TEFs result from a variety of causes. Among these causes, the most common is iatrogenic that results from prolonged tracheal intubation. Denture impaction of the esophagus resulting in the development of an acquired TEF is rare. Whatever be the cause, the diagnosis of a TEF is a surgical emergency because delay in treatment can result in devastating pulmonary complications from aspiration through the TEF. Surgical treatment of non-malignant TEFs usually gives good results. An unusual case of non-resolving pneumonia resulting from recurrent aspiration through an acquired TEF caused by an accidentally swallowed denture is reported here. Patient's pneumonia resolved completely following the surgical correction of the fistula.Keywords: Denture, non-resolving pneumonia, tracheo-esophageal fistula INTRODUCTION The majority of cases of acquired tracheo-esophageal fistulas (TEF) result from malignancy.[1] Iatrogenic injury from prolonged tracheal intubation is the commonest cause of non-malignant acquired TEF.[1],[2] Diagnosis of a TEF warrants urgent surgical intervention because the delay in treatment can cause catastrophic pulmonary complications resulting from aspiration through the TEF. Denture impaction of the esophagus resulting in an acquired TEF has been very rarely reported in the literature and such a case poses much diagnostic and therapeutic difficulties.[3] Esophageal impaction of an accidentally swallowed denture causing an acquired TEF and non-resolving pneumonia and its surgical correction is reported here. CASE REPORT A 20-year-old male was admitted for evaluation of cough and loss of weight for two months. He reported that the cough would become more severe while taking food, especially liquids. He tried to avoid drinking fluids for fear of getting bouts of cough and the reduced food intake was accompanied by a weight loss of 6 kg. He had epilepsy in the previous 6 years, which had been inadequately controlled owing to poor compliance to antiepileptic medication. Multiple courses of antibiotics before admission, with a clinical and radiological diagnosis of left lower lobe pneumonia, had given little relief to the cough. Clinical examination revealed anemia and coarse crackles in the left infra-scapular and infra-axillary areas. Chest radiography confirmed the clinical diagnosis of left lower lobe pneumonia [Figure - 1]a. No other abnormalities were revealed in the preliminary clinical and laboratory evaluation. A bronchoscopy was performed to exclude the possibility of a tumor or inhaled foreign body causing non-resolving left lower lobe pneumonia. It showed a fistulous opening at the lower end of trachea ([Figure - 2]a, white arrow). A biopsy from that site revealed non-specific inflammation only. Esophagoscopy and barium esophagography [Figure - 1]b confirmed the presence of a TEF. Further probes into the patient's history revealed that he had started getting the coughs a few days following an episode of generalized seizures. He had been missing a denture following the seizures. The patient was taken up for surgery and through a cervical approach the fistula was dissected. The impacted denture was removed ([Figure - 2]b, black arrow) after separating the trachea from the esophagus. Tracheal and esophageal ends of the fistulous track were freshened. The tracheal end was sutured horizontally with interrupted vicryl sutures (coated with polyglactin). The esophageal end was also sutured in two layers with the same material. A pedicled strap muscle flap was inter-positioned between the trachea and esophagus and was held in place with coated polyglactin suture in order to reinforce the closure for prevention of recurrence of the fistula. The wound was closed with suction drain. After surgery, the pneumonia resolved completely and he regained his original weight within a period of two months. DISCUSSION A majority of the cases of acquired TEFs are a result of complication of malignancy. The tumors of the esophagus, lung, trachea, larynx, thyroid, and lymph nodes can cause TEF.[1] Acquired non-malignant TEFs result from a variety of causes such as iatrogenic injuries, granulomatous infections (tuberculosis, histoplasmosis, candidiasis, syphilis, and actinomycosis), inflammations (Crohn's disease and Behcet's disease), blunt and penetrating chest trauma, ingestion of foreign bodies and corrosives, AIDS, prior esophageal and tracheal surgery, and indwelling stents. The most frequent cause of acquired non-malignant TEF is iatrogenic and results from prolonged tracheal intubation.[1],[2] Impacted denture as a cause of acquired non-malignant TEF is rare and poses much diagnostic and therapeutic challenges.[3] In clinical practice, the most commonly encountered esophageal foreign bodies in adults are impacted meat or bones. Use of dentures increases the risk of impaction because they decrease the palatal sensations leading to misjudging of the size of the swallowed bolus of food. Impaction usually occurs at the cricopharynx and the removal of the object if delayed, may result in local necrosis and formation of a TEF. Swallowing dentures and dental plates has been a cause of distress among elderly patients and may result in a TEF if the denture gets impacted in the esophagus.[3] Regardless of the etiology, the sequelae of the TEF are the same: tracheobroncheal contamination with significant pulmonary compromise and inadequate nutrition.[1] Symptoms and signs are due to the increase in tracheal secretions and aspiration during swallowing resulting in paroxysms of cough and recurrent pneumonia. Patients may try to avoid food and drinks for fear of choking spells and may report presence of food particles in the expectorated material. Bronchoscopy, esophagoscopy, fistulography, and computed tomography might aid the diagnosis of TEF but clinical suspicion in a patient at high risk is more crucial considering increased morbidity and mortality in cases of delayed diagnosis and treatment. Once diagnosed, surgical correction of acquired TEF is usually required because spontaneous closure is rare and the delay in repair is hazardous. Surgical repair usually gives good results in acquired TEF resulting from non-malignant diseases and recurrences are rare.[4],[5] Tracheo-esophageal fistula from malignancy, which accounts for more than 50% of acquired TEFs, is a devastating complication. It can't be cured because of the underlying incurable disease process and the most effective treatments are esophageal bypass and esophageal stenting.[1] References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07006f1.jpg] [is07006f2.jpg] |
| |||||||||

{kind=link}
{kind=link}