 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
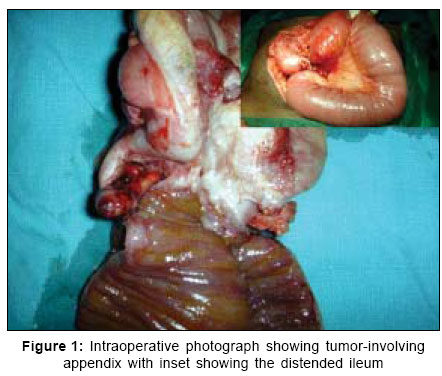
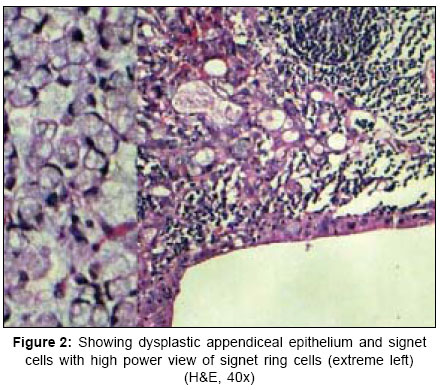
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 22-24 Case Report Signet ring cell carcinoma of the appendix presenting with intestinal obstruction Arcot Rekha, Thanka J, Rajendiran S, Ravi A Sri Ramachandra Medical College and Research Institute, Deemed University, Porur, Chennai Code Number: is07007 Abstract Appendicular carcinomas are rare tumors. They are more likely to be carcinoids, mucocoeles and adenomas. Signet ring cell carcinoma is uncommon in the appendix. We report our patient who presented with intestinal obstruction due to a signet ring cell carcinoma of the appendix, (studies proved that it was not a primary colonic lesion invading the appendix) and review literature of this very uncommon lesion.Keywords: Appendix, obstruction, signet ring cell carcinoma INTRODUCTION Neoplasms of the appendix are rare lesions. Most of the appendiceal tumors are adenocarcinomas or carcinoids. The appendix can also be the site of metastases from the breast, the ovary, the gastrointestinal, and the female genital tract. There are few reports of primary signet ring cell carcinoma arising from the appendix, but a search of literature showed no report of the carcinoma presenting as intestinal obstruction. CASE REPORT A 42-year-old well nourished male patient presented to the surgical outpatient department, with features of sub acute intestinal obstruction-he had intermittent vomiting, abdominal distension and episodes of obstipation, which would resolve spontaneously. Examination of the patient showed no anemia, icterus, lymphadenopathy or pedal edema. Examination of the abdomen revealed a mass in the right iliac fossa, 5x3 cm and firm in consistency with no pulsation or cough impulse. The total WBC count was elevated, the ultrasound showed a mass lesion in the right iliac fossa, with focal dilated bowel loops, Mantoux skin test was non-reactive and the erythrocyte sedimentation rate was 6/11. An initial diagnosis of appendicular mass was made and the patient started on Oshner Sherren regimen. Patient failed to respond significantly and at the end of the first week, a CT done showed a mass lesion in the region of cecum, with proximal dilated bowel loops. At laparotomy, through a lower mid line incision, we found a mass formed by the cecum, the terminal ileum, the proximal ascending colon engulfing a turgid appendix [Figure - 1] in a pre-ileal location. The ileum proximal to the mass was distended ([Figure - 1]-inset). There were several nodes all over the mesentery and several nodules over the parietal and visceral peritoneum and also over the bladder and the liver. In view of the extensive nodal involvement, a frozen section (of the peritoneal nodule) was sent. The report was signet ring cell carcinoma. We proceeded with a right hemicolectomy with ileotransverse anastomosis. The patient recovered well after the procedure. Histopathology The gross specimen showed a thickened appendix, with a solid grey white tumor in the base protruding into the cecal mucosa causing a pebbled appearance. There were nodules present over the serosa of the colon as well as the mesentery. Microscopy showed signet ring cell carcinoma of the appendix, predominantly involving the full thickness of the wall. The mucosa overlying the tumor showed dysplastic changes. While the appendiceal mucosa showed dysplastic changes the colonic mucosa was free, thus suggesting primary appendicular tumor [Figure - 2]. The tumor was also seen extensively involving colonic muscle layer, serosa, and mesentery. The margins of resection were free of tumor. The malignant cells within the nodules show variable intercellular adhesion and had the characteristic features of malignant signet ring cells: scant cytoplasm stretched over an intracytoplasmic mucin droplet and an eccentric, crescentic nucleus pushed at the periphery of the cell by the mucin vacuoles ([Figure - 2]-inset). To rule out the possibility of metastatic signet ring cells, immunohistochemical stains for CK20 were performed the signet ring cells were positive for CK20 (immunoprofile that confirms their intestinal origin). The tumor cells were positive for cytokeratin and negative for chromogranin and synaptophysin thus confirming signet cell carcinoma and excluding goblet cell carcinoid. The patient was referred to the oncologist and was started on chemotherapy with lavamisole and fluorouracil. In view of the advanced nature of the disease, patient tolerated chemotherapy poorly and died within six months. DISCUSSION Appendiceal tumors are uncommon and often present as appendicitis.[1] Benign lesions include adenoma, cystadenomas, mucinous cystadenomas, appendiceal neuromas, mucinous hyperplasia, and mucocoele. The malignant tumors of the appendix are adenocarcinomas, carcinoids, mucinous cystadenocarcinoma, pseudomyxoma peritoneii, and secondaries in the appendix.[1],[2],[3] Rare tumors of the appendix include signet ring cell carcinoma, goblet cell carcinoid, small cell carcinomas, gastrointestinal stromal tumors, and lymphomas.[1] Primary appendiceal tumors are also reported to have metastasized to the ovaries.[4] Signet cell carcinoma of the colon is rare, representing less than 2% of all colonic adenocarcinomas. Signet cell carcinoma of the appendix is rarer, and associated with a poor prognosis. Signet cell carcinomas of the appendix are staged according to the TNM classification. Like carcinoma anywhere in the colon, the treatment is resection of the tumor. There are no previous reports of appendicular SRC presenting with intestinal obstruction. There are few reports of gastric signet cell carcinoma with loss of E cadherin.[5] Since there are no studies comparing the advantage of any surgical procedure due to the paucity of cases, most surgeons prefer a right hemicolectomy as the treatment of choice. During a 16 year period study there was only 0.9% incidence of appendiceal tumors and only 0.1% of malignant tumors.[1] There is also a record of abdominal wall metastases arising from a signet cell carcinoma of the appendix and a patient with mucinous cystadenoma of the appendix presenting with intestinal obstruction.[6],[7] One paper reports four patients with mixed adenocarcinoma and carcinoid. Immunohistochemistry is useful in differentiating these tumors from other mucous secreting lesions.[8] The E-cadherin shows variable staining pattern ranging from continuous, weak membranous staining to discontinuous staining to completely absent labeling in the discohesive single signet ring cells desquamated into the luminal space. This staining pattern suggests that the loss and partial loss of E-cadherin cell-adhesion molecule may be responsible for the discohesive quality of the signet ring cells, which in turn may play a role in the tumor progression. This has been previously demonstrated in signet ring carcinoma of the stomach.[5] Signet cell carcinomas are often seen in the stomach and colon. Appendicular neoplasm are uncommon lesions, more so signet ring cell carcinoma of the appendix. We report an advanced signet ring cell carcinoma with multiple metastases and dissemination presenting with intestinal obstruction, as it has not been previously reported. Signet cell carcinomas of the appendix are very often associated with a poor prognosis as is in our patient. References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07007f2.jpg] [is07007f1.jpg] |
| |||||||||

{kind=link}
{kind=link}