 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
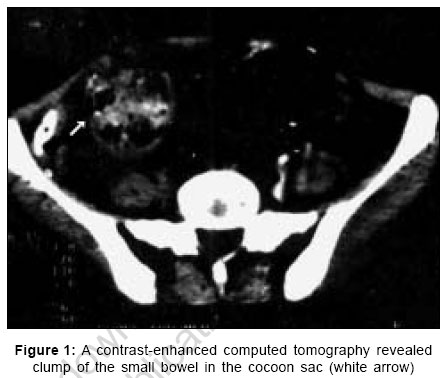
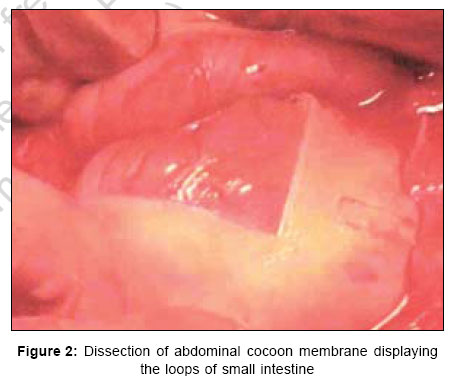
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 25-27 Case Report Abdominal cocoon in identical twins: Is it congenital collagen tissue disorder? Report of two cases with review of literature Srivastava Pankaj, Sahu Manoranjan S. S. Hospital, Varanasi, Uttar Pradesh Code Number: is07008 Abstract Abdominal cocoon (AC) is a rare disease entity most often found in adolescent girls from tropical and subtropical countries. The etiology is largely unknown. We report herein our experience of two cases of AC detected first time in identical female twins in the literature so far. One presented with acute intestinal obstruction and another asymptomatic one was evaluated on the basis of high index of suspicion and was operated for the same. Recovery was uneventful in both the cases. It is also hypothesized that the AC could be considered as congenital collagen tissue disorder, having some genetic predisposition. To the best of our knowledge, there are no reported cases within the same family. In addition, it has not been identified in subsequent generations, making a single gene mutation unlikely.Keywords: Abdominal cocoon, collagen disorder, intestinal obstruction, peritonitis INTRODUCTION We report herein abdominal cocoon (AC) first time in identical female twins in which it is emphasized that the individuals with AC may have a genetic susceptibility to developing the condition and the AC may be a pathological progression from a congenital abnormality of the peritoneum. In a relatively recent review, a total of 40 cases of primary AC have been reported since it was first described in 1978.[1],[2],[3],[4] CASE REPORTS Case 1 An 18-year-old young girl, one of the identical twins was presented with colicky abdominal pain, vomiting, low-grade fever, and absolute constipation for two days. She had had similar attacks of abdominal pain and vomiting associated with abdominal distension and constipation for last three years. She had no significant past history. She had started menarche two years ago. On physical examination, pulse was 110/minute oral temperature was 100.4°F and blood pressure was 100/70 mmHg. General and systemic examination revealed no abnormality. Local examination revealed large, globular, tender abdominal swelling with ill-defined margins and restricted mobility in the umbilical region extending to the right iliac fossa. Percussion note was tympanic. The bowel sounds were increased and high-pitched. Routine investigations were normal. Abdominal radiograph showed multiple air-fluid levels. Ultrasonography also confirmed small bowel obstruction. After gastric decompression with nasogastric tube and a period of rehydration, under general anesthesia, exploratory laparotomy was performed through a right paramedian incision. After opening the peritoneum, a large, globular, glistening white, bag-like swelling, occupying the central abdomen was noticed. The swelling was covered by a thick, fibrous membrane encasing the small bowel from the duodenojejunal junction to the terminal 4-5 cm of the ileum. The whole mass was freely mobile, being free from the parietal peritoneum. In the right lower quadrant there was a small, non-constricting aperture in the sac from which the terminal ileum emerged. At this point, membrane was incised and the small bowel exposed itself. The whole of the small intestine within the fibrous membrane was coiled up in concertina-like fashion. The coils of intestine were collapsed and separated easily from each other with the intestinal serosa intact. The complete small bowel freed from the fibrous membrane, was viable and required no more surgical procedure. The post-operative period was uneventful. Follow-up was maintained for two years with no complaints except that the keloid was developed in her abdominal scar. Histopathologic study of the membrane revealed non-specific inflammatory changes with fibroblastic proliferation. The membrane was composed of thick collagenous fibrous tissue. Case 2 On the basis of high index of suspicion, another of the above identical twins was also evaluated. She was asymptomatic otherwise but she had history of abdominal pain intermittently for last one year. On examination, ill defined, non-tender, freely mobile, globular mass, occupying the central abdomen was noticed. She had also no significant past history. She had started menarche two years ago. Abdominal radiograph showed remarkable appearance of the small bowel loops. Abdominal ultrasound showed small bowel loops encased in a thick fibrous membrane with minimal fluid collection in the pelvis. A contrast-enhanced computed tomography of the lower abdomen revealed clump of small bowel with loculated fluid, limited by a well-defined sheath [Figure - 1]. An elective laparotomy revealed dense generalized membranous adhesions encasing the whole of the small intestine from the duodenojejunal junction to ileocecal junction. The rest of the findings were similar to the above case. Adhesiolysis was done using a combination of blunt and sharp dissection [Figure - 2]. After freeing the loops of small intestine, no more surgical procedure was required. The recovery was uneventful. Follow-up was maintained for two years with no complaints except that the keloid was developed in her abdominal scar. Histopathologic study of the membrane revealed collagenous fibrous tissue all over the membrane with no features of inflammation. DISCUSSION The exact aetiology of AC is still obscure. Retrograde menstruation coupled with viral infection, once theorized by Foo et al .[4] as a possible etiology, does not explain the occasional occurrence of AC in males[5],[6] and in children.[7],[8] In our study, though the age and sex may favor this theory, the occurrence of retrograde menstruation with superimposed viral infection concurrently in the identical twins is impractical. The absence of lymphocytes and plasma cells in the cocoon membranes of both the cases and non-inflammatory nature of membrane in the second case further conflict the above hypothesis. Review of literature suggests chronic inflammation as a major factor in the pathogenesis of the AC but the second case in our report conflicts that, because no features of inflammation could be detected clinically or histologically though the operative findings were almost similar except the absence of intestinal obstruction. The features of inflammation in previous reports and in the first case could be due to small bowel obstruction. It is further conflicted with the fact that the cocoon is often separated from the parietal peritoneum, which suggests that the pathology of the AC is other than chronic inflammation. The occurrence of AC in both of the identical twins with abundance of collagen tissue detected on histopathologic studies of cocoon membranes gives an idea regarding the possible etiology that the AC could be a congenital collagen tissue disorder having some genetic predisposition. The presence of collagen balls in the ascitic fluid cytology with AC signifies the role of collagen in the pathogenesis.[9] The development of keloid scar in both the patients postoperatively also favors the above etiology.[10] The keloid scars were also described in the four out of ten cases by the Foo et al .[4] The consistent presence of the lesion with invariable involvement of the ileocecal junction supports the idea of a developmental abnormality. The present report also favors the developmental abnormality. It is hypothesized that the 'AC' is a developmental malformation with some genetic predisposition in which, collagen tissue disorder plays key role in the formation of encapsulating membrane around the small bowel. This hypothesis needs further work to explain the exact etiology. References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07008f2.jpg] [is07008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}