 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
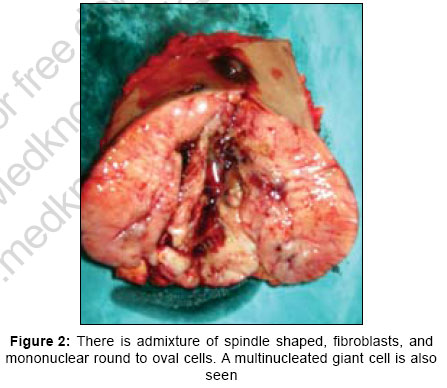
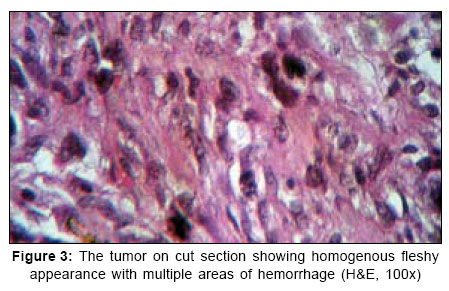
Indian Journal of Surgery, Vol. 69, No. 1, January-February, 2007, pp. 28-30 Case Report Primary malignant fibrous histiocytoma of the breast Singh Karam, Singh Kuldeep, Singh Amritpal, Rajan, Singh Gunjit, Singh Rajbir Department of General Surgery, Govt. Medical College/Rajindra Hospital, Patiala, Punjab Code Number: is07009 Abstract Sarcomas of the breast are uncommon, accounting for less than 1% of all primary malignancies. Among these tumors, malignant fibrous histiocytoma (MFH) is very rare. One case of the MFH of the mammary gland is presented in this paper. A 20-year-old unmarried female presented with a left breast lump. Fine needle aspiration cytology was inconclusive. Biopsy revealed the diagnosis of malignant phylloides tumor. After simple mastectomy, histological diagnosis of MFH was made. In addition, the possibilities of the therapy of the MFH in the breast are discussed.Keywords: Histiocytoma, mammary gland, malignant INTRODUCTION Malignant fibrous histiocytoma (MFH) is a soft tissue tumor with poor prognosis, representing the most common soft tissue sarcoma of middle and late adulthood.[1],[2] The lower and upper extremities are most frequent site, but occurrence in breast is very rare.[1] MFH is also known as malignant fibrous xanthoma, pleomorphic fibrous histiocytoma and pleomorphic fibrous xanthoma.[1],[3] In this case report, we present a 20-year-old unmarried female with MFH involving left breast. CASE REPORT A 20-year-old unmarried female was admitted in emergency with a diagnosis of breast abscess having a swelling in upper and outer quadrant of left breast. She had first noticed the swelling two months back, since then it had grown rapidly. There was no history of fever, pain, weight loss, loss of appetite or discharge from nipple. On examination, skin over swelling was tense, glossy, and erythematous with dilated subcutaneous blood vessels [Figure - 1]. On palpation swelling was found to extend to other quadrants of breast also but nipple areola complex was normal. Swelling was about 86 cm in size, was non-tender with irregular surface and well defined margins. It was freely mobile over underlying structures. Temperature of skin overlying swelling was not raised. No lymph node was palpable in left axilla. Patient was put on antibiotics but there was no response to treatment. On the contrary swelling increased in size during the stay in the hospital. Patient was severely anemic and was given blood transfusion. White cell counts and X-ray chest was normal. Ultrasonography (USG) abdomen was normal expect for a small right ovarian cyst. On fine needle aspiration cytology (FNAC) no pus could be aspirated rather a serosangious fluid came out with bleeding at the site of needle prick. USG of left breast revealed a large hypoechoic mass with multiple cystic areas, most of them with internal echoes visualized involving all quadrants of breast, more so on lateral aspect. Some of them have internal septations. A provisional diagnosis of breast abscess was suggested on USG. However, FNAC findings were compatible with phylloides tumor with foci of suspicious look. Therefore, biopsy was taken under local anesthesia that suggested the diagnosis as malignant phylloides tumor with differential diagnosis of fibrosarcoma. Simple mastectomy under a general anaesthetic was performed. On gross examination the excised specimen showed homogenous fleshy appearance with multiple areas of hemorrhage. Wound left open, as closure was not possible due to wide excision. Histopathological examination showed a tumor of 12x8x4 cm in size. The margins were clear. Microscopic examination showed admixture of spindle shaped fibroblasts and mononuclear histiocyte-like cells [Figure - 2]. At places storiform pattern and other places, spindle cells intersecting about a center focus, were present. There was high degree of nuclear atypia. At places areas of hemorrhages and necrosis were seen. These features were strongly suggestive of MFH [Figure - 3]. The wrong histopathological diagnosis on open biopsy earlier could be due to paucity of tissue taken on open biopsy.The pathologist found only features suggested of phylloides tumor in that specimen. It became possible to label the tumor as MFH only after whole of the tumor was seen under microscope. After two weeks patient underwent superficial skin grafting of wound by plastic surgeon. The wound healed in about 12 days. The patient was subsequently discharged and referred to radiotherapy department for further management. However, the patient did not report back to radiotherapy department after her first visit. DISCUSSION Primary malignancies of breast stromal elements and sarcomas of mesenchymal origin comprise less than 1% of all breast neoplasms and are a highly heterogeneous group of tumors. This diverse group includes MFH, fibrosarcomas, liposarcomas, and angiosarcomas.[4] MFH arises most frequently (58-75%) from the deep fascia or skeletal muscle of the limbs and then occurs frequently in the retroperitoneum and abdominal cavity with a frequency of 9-16%. Also found to occur in mediastinum and bones. However, its development in breast is extremely rare. Youngest age ever reported in the literature with MFH is 14 years. Histologically, the essence of MFH is pleomorphism that contains two types of cells: fibroblast-like cells and histiocyte-like cells. Each tumor contains varying proportions of the two cell types so that a wide range of histological features is possible.[2] As a result, MFH have been characterized into following subtypes: storiform pleomorphic, myxoid, giant cell, inflammatory and angiomatiod. For proper management and prediction of prognosis, differentiating MFH from other carcinoma or sarcoma is very important. Differential diagnosis of MFH includes cystosarcoma phylloides, pleomorphic rhabdomyosarcoma and spindle cell carcinoma. Metastases of MFH are mainly hematogenous to lungs and lymph node involvement is very unusual. In addition, the tumor is prone to local recurrence. When the involvement of lymph node is present, it is considered as a sign of widely disseminated disease.[5] For reason, axillary node dissection has not generally been recommended in the treatment of this tumor.[3] However, clarifying lymph node status by dissection is useful for predicting the prognosis and helping to determine the indications for the post-operative adjuvant therapy. Consequently, it will be up to the surgeon in case-by-case matter to decide whether axillary dissection is necessary or not. In terms of the post-operative adjuvant therapy, radiation therapy seems to play an important role.[6] The effect of chemotherapy, however, is still uncertain. But some have claimed success with adriamycin. In general, prognosis of MFH is poor due to local recurrence and if lymph node involvement is present. The most important prognostic factor is the depth of location, followed by size. In spite of its rarity, surgeons should be alert to the existence of this type of soft tissue tumor in the breast. A pre-operative core biopsy sometimes misleads about the diagnosis, as one of the differential diagnosis of MFH is cystosarcoma phylloides. So far, surgery is the first step in the treatment. Although it remains doubtful whether radical or modified radical mastectomy is superior to wide local excision, the important point is to secure safe surgical margins of more than 3 cm,[7] in which ever procedure that would be carried out. References
Copyright 2007 - Indian Journal of Surgery The following images related to this document are available:Photo images[is07009f2.jpg] [is07009f1.jpg] [is07009f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}