 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Applied Sciences & Environmental Management, Vol. 6, No. 1, June, 2002, pp. 5-7 The Effect of Alcohol on Uric Acid Level in Consumers *BARTIMAEUS, E. S; ENO-ENO, M. Department of Medical Laboratory Sciences,
Rivers State University of Science and Technology,
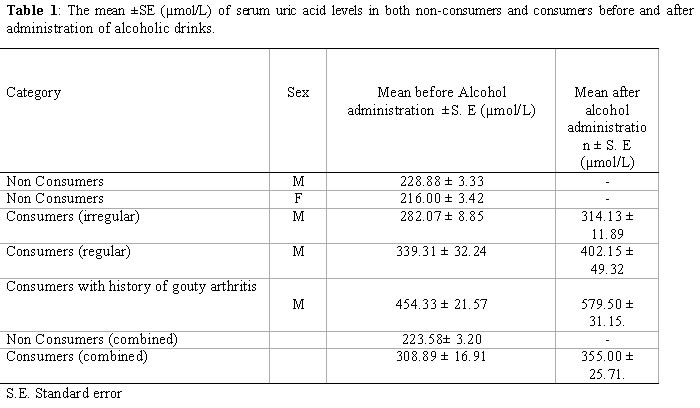
P.M. B 5080, Nkpolu, Port Harcourt, Rivers State. Code Number: ja02001 ABSTRACT: The effect of alcohol in uric acid level was investigated in regular and irregular alcohol consumers who were mainly males. The result showed that the mean (±SE) of non-consumers of alcohol and consumers (combined) was 228 ±3.32 µmol/L and 308.89 ±16.91 µmol/L respectively and the means were significantly different at p<0.05. The mean uric acid level in irregular consumers before administration of alcohol and that after administration was 282.07 ±8.85 and 314. ±11.89 µmol/L respectively. The mean uric acid level in regular consumers and irregular consumers with history of gouty arthritis before and after administration of alcohol were 339.31 ±32.24 µmol/L, are 454.33 ±21.57 µmol/L and 402. 15 ±49.32 µmol/L and 579.50 ±31.15 µmol/L respectively. Comparison of mean values before and after alcohol intake between these categories were significant at p<0.05. The effect of alcohol on the increased uric acid level in both regular and irregular consumers shows significance at p<0.05.@ JASEM Uric acid is a waste product derived from purines in the diet and those synthesized in the body (Tietz, 1982). Hyperuricaemia or elevated serum levels of uric acid is usually encountered in various clinical situations involving the net degradation of ATP (Fox, 1985). Determination of blood uric acid levels are most helpful in the diagnosis of gout in which although occasionally normal serum uric acid levels may be found, repeated examination will usually reveal hyperuricaemia at some point in the disease (Tietz, 1982). Alcohol consumption has traditionally been associated with hyperuricaemia and in susceptible persons, the precipitation of acute gouty arthritis (Wyngaarden and Kelly, 1976). This study therefore was designed to investigate the effect of some locally consumed alcoholic beverages on serum uric acid level among consumers in Port Harcourt metropolis, Rivers States. MATERIALS AND METHODS Forty individuals of age ranging between 26 - 62 years residing in Port Harcourt volunteered and participated in the study. Amongst them were 15 regular alcohol consumers, 13 irregular consumer out of which 6 have diagnosis of gouty arthritis and 12 non - consumers of any alcohol beverage. The regular and irregular consumers were instructed to abstain from drinking three days prior to the day of test. On the day of the test an initial blood sample was collected from all the 40 participants. The 28 regular and irregular consumers were then offered according to their preferences three bottles of either gulder or star lager beer. Three of the regular consumer preferred reasonable short of local alcohol (ogogoro or khai khai) to the lager beer. One hour after consumption of the alcohol, another blood sample was collected from the 28 regular and irregular consumers. Blood samples were collected by venepuncture, centrifuged for 5 minutes at 3,000 rpm using MSE centrifuge and put into plain sterile sample bottles and analyzed within 1 hour after collection. The method of Cheesbrough (1987) was used in the estimation of uric acid in the serum. The normal ranges of uric acid for the method used were: Men, between 202-416µmol/L and Women, between 142-339 µmol/L. The data were subjected to analysis of mean and student t-test to test for significant differences in means before and after alcohol administration. The effect of alcohol on increased uric acid level was tested using the paired sample t - test. Values were considered significant at p < 0.05. RESULTS AND DISCUSSION The serum uric acid level in both non consumers and consumers of the alcoholic beverage before and after administration of alcoholic beverage are shown in table 1 The table shows that the mean serum uric acid level in the consumers (males) was 228.88 ± 3.33 µmol/L. The mean level of uric acid in irregular consumers before administration of alcohol was 282.07 ± 8.85 µmol/L and 339.31 ± 32.24 µmol/L for regular consumers while mean levels after alcohol intake were 314.13 ± 11.89 and 402.15 ± 49.32 µmol/L for irregular and regular consumers respectively. Subjects with history of gouty arthritis showed mean level of 454.33 ± 21.57 and 579.50 ± 31.15 µmol/L before and after alcohol intake. The mean uric acid level for non-consumers of alcohol (combined) and consumers (combined) before alcohol intake was 223.58 ± 3.20 and 308.89 ± 16.91µmol/L respectively. The mean level of uric acid in non consumers (combined) was compared statistically with the mean level of uric acid in consumers (combined) before intake of alcohol using the student t-test and was found to be significant at p<0.05. Similarly, the mean uric acid levels in the regular, irregular and consumers with history of gouty arthritis before and after alcohol intake were also compared. Results showed that there were significant differences between means in the regular consumers and those with history of gouty arthritis before and after alcohol intake at p<0.05 while irregular consumers did not show significant difference in mean before and after alcohol intake. The effect of alcohol consumption on the increase in uric acid level in regular and irregular consumers after drinking alcohol was investigated using the paired sample t-test and the increase was shown to be significant at p<0.05. The increase in uric acid level in subjects with history of gouty arthritis following alcohol intake was also significant at p<0.05. The uric acid level in the male alcohol consumers (regular and Irregular) before administration of alcohol was 308.89±16.91 µmol/L while the mean of 228.88 ± 3.33 µmol/L was obtained for male non -drinkers. These means were statistically significant and different at p<0.05. Even though the increased level was high normal, the study shows that in susceptible persons exposed to alcohol consumption, the rise could be tremendous and diagnostic. This was the opinion of Wyngaarden and Kelly (1976) who reported that alcohol consumption has traditionally been associated with hyperuricaemia and in susceptible persons, the precipitation of acute gouty arthritis. The effect of alcohol consumption on the serum uric acid level of both regular and irregular consumers shows a consistent increase and when investigated using the paired sample t-test to prove the dependence of the increase on alcohol consumption, the correlation was significant at p<0.05. In the other words, alcohol consumption has a direct effect on uric acid elevation. In the regular alcohol consumers, a 10.8 to 28 per cent increase in serum uric acid level was observed while in the irregular alcohol consumers a 2 to 7 per cent was observed. This finding agrees with the work of Whitehead et al (1978) who stated that as a result of the efficiency of alcohol to cause a rise in serum uric acid level, it could be recognized as a biochemical marker for hyperuricaemia. The present study also showed that subjects with history of gouty arthritis who romances with alcohol precipitate significant increases in serum uric acid level. Saver et al (1967) and Gibson and Graham (1974) had reported high prevalence of gouty arthritis amongst regular alcohol consumers and populations with a high prevalence of gouty arthritis have a high population of excessive drinkers. In this study the authors believed that patients with history of gouty arthritis who are involved in consumption of alcoholic beverages of any type risk the chances of precipitation of the disease due to increase in the precipitation of uric acid levels observed as indicated in this study. However, this study is limited by the small sample size, our inability to specify the proportion of increase contributed by specific alcoholic beverage, and the short exposure time to the alcohol during the study. Since excessive alcohol consumption is fast becoming a part of the Nigerian society, the effect of alcoholic consumption on the life of consumers warrants additional and further investigation. REFERENCES.
Copyright 2002 - Journal of Applied Sciences & Environmental Management The following images related to this document are available:Photo images[ja02001t1.jpg] |
| |||||||||
{kind=link}