 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Applied Sciences & Environmental Management, Vol. 6, No. 1, June, 2002, pp. 69-72 Effect of Caffeine on the Polymerization of HbS and Sickling Rate/Osmotic Fragility of HbS Erythrocytes *UWAKWE, A A, ONWUEGBUKE, C; NWINUKA, N M Department of Biochemistry, Faculty of Science, University of Port Harcourt, P. M. B. 5323, Port Harcourt, Nigeria
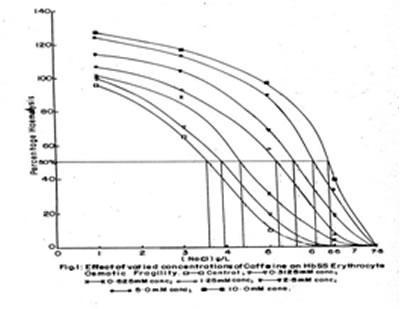
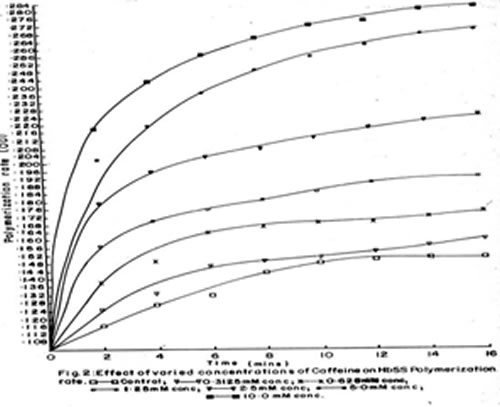
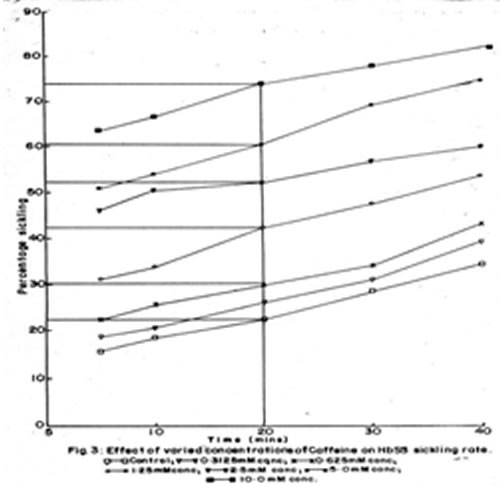
Code Number: ja02015 ABSTRACT: The effect of exogenous caffeine on human hemoglobin-S (HbS) erythrocytes was investigated in vitro, using caffeine concentrations in millimole per liter (0.0mM-10mM) on three criteria; osmotic fragility, sickling rate and polymerization effects. The determinations were carried out on different age groups from infancy through adolescence. The result obtained demonstrated that caffeine could hasten sickling as well as fragility of HbS erythrocytes in a concentration - dependent manner. For instance at an optimum caffeine concentration of 10mM and saline concentration of 5g/l, red cell lysis increased by 90% relative to the control (0.00mM caffeine). At the same optimum concentration of 10mM, caffeine also increased HbS erythrocyte sickling and HbS gelation by 65.00% and 83.78% respectively after 10 mins of incubation with 2% sodium metabisulphite. Based on these observations; caffeine concentration in plasma might proffer marked increase in erythrocyte sickling in vivo, and consequently, slow recovery from a sickling crisis. This result could prove useful towards the management of sickle call disease (SCD). @ JASEM Sickle cell hemoglobin (HbS) is a type of abnormal hemoglobin occurring in the erythrocytes of sickle cell disease (SCD) (hemoglobinopathic) subjects, provoking sickling of erythrocytes into elongated crescent shape, a change from the normal bi-concave disc upon deoxygenation. The end result is polymerization into crystals (Wishner et al 1975, Luzzatto, 1981). The resultant sickle erythrocyte deformity produces the most remarkable cause of all the crises experienced by SCD subjects (Hebbel et al 1981). With the understanding of sickle cell hemoglobin as a genetic complication, the management of SCD in the present time, is widely towards general supportive therapy and treatment of sequential disorder (Charache et al, 1984). In recognition of this, experimental studies have been done in recent years exploring certain foods, food and drug additives or constituents (Ekeke and Diogu, 1989, Ekeke and Ibeh, 1988, Ekeke and Nsirim, 1987). This evokes our investigation on caffeine, an alkaloid related to purine, being used as drug or its constituents and in some foods of which less is known about its activity in sickling. Caffeine (1, 3, 7 - trimethylxanthine) was first isolated from coffee in 1820(Arnand, 1984). It was subsequently identified in cocoa, mate, kola nuts and other plants. Caffeine is one of several methylxanthines, that occur naturally, primarily in plant matter, that is used to prepare beverages. The methylxanthines, as dioxypurines, are related to the nitrogenous compounds - adenine and guanine, a property that is relevant to their biosynthesis and physiological effects (Harold, 1992). In addition to its natural occurrence, caffeine is added to the very widely consumed cola drinks and other soda products. This usage is based on its stimulatory properties and the slight degree of bitterness that it imparts (Harold, 1992). The purpose of this work is to evaluate the effect of caffeine on the polymerization of HbS; the HbS erythrocytes sickling rate and the HbS erythrocytes osmotic fragility; and its possible role in SCD management. MATERIALS AND METHODS Caffeine: This was extracted from Nescafé(k)(product number CC5AA) a brand of "instant coffees" Produced By Nestlé Foods, Lagos, Nigeria using Harris method adapted from FDALS (1982) and confirmed by Wagenar test (Arnand, 1984). Sodium chloride, and Sodium metabisulphite were purchased from Sigma Chemical Company U. S. A. Blood Collection: The blood samples were collected from UNIPORT and UPTH students and patients. The HbSS status were formally confirmed from the sampled subjects by UPTH laboratory technologists using standard Hb electrophoresis. The subjects were aged between 31/2 and 26 years, and of both sexes. The blood samples used for all tests were collected in heparin bottles for non-coagulation and were used fresh within 5hrs after collection. PROCEDURE Caffeine dilutions: 0.03g of pure caffeine previously extracted was dissolved in 12.5ml distilled water to produce 10mM. From this stock solution, various dilutions of 5mM, 2.52mM, 1.25mM, 0.635mM and 0.3125mM were made to simulate similar concentration in foods and drugs. Haemoglobin preparation:For polymerization test, uncoagulated HbS erythrocytes were left to thaw through which haemloysis occurred. On adding distilled water and centrifuging at 3500 rpm for 5 mins at 37°C, the sickle haemoglobin sedimented while the supernatant, plasma and ghost cell were carefully drawn out using Pasteur pipette. The required haemoglobin - S was produced by dilution of 1:2 v/v with 0.9% w/v normal saline. Polymerization Action: This was carried out using the method described by Noguchi and Schechter (1985). 0.5ml of 0.9% w/v normal saline was each added to test tubes containing various dilutions of caffeine of 0.1ml respectively. 4.4ml of freshly prepared 2% w/v aqueous sodium metabisulphite (Na2S202) and 0.1ml of HbS were added into the tubes simultaneously. The contents were mixed and the optical density (O.D) read from the spectrophotometer at 700nm, after standardizing with blank of distilled water. Readings were taken for a period of 16 mins at 2mins intervals. Appropriate control experiment was set up excluding caffeine addition. Osmotic Fragility Effect: This was carried out using the method described by Dacie et al (1981). Exactly 5.0ml each of saline solutions - 9.0, 7.5, 6.3, 5.6, 3.5, 1.0 g/1NaC1- were delivered into 1x12cm test tubes. In the 7th tube, 5.0ml distilled water was added. To these tubes 50 m1 of well mixed fresh blood were added respectively. The whole mixtures were thoroughly but carefully mixed to avoid foaming. After incubation at room temperature for 30 mins, the mixtures were each mixed again before centrifugation at 1200g for 5mins. Using tube 1 supernatant (osmotically equivalent to 9.0g/l NaCl) as blank, the supernatants were decanted and colorimetrically estimated, by OD, for the amount of lysis in each tube at 540nm. This served as the control experiment. Test experiments were carried out by repeating the procedure at 0.1ml of different test concentrations (0.3.125,0.625,2.5.5.0 and 10.0mM) of caffeine. Red Cell Sickling Effect: This was carried out using the method described by Daland and Castle (Daland and Castle, 1984). The test was prepared and observed under the microscope (x 100). For each of the caffeine concentrations described above 0.1ml of freshly prepared 0.9% w/v saline and 20%w/vNa2S2O5 were dropped on a slide (Daland and Castle, 1984). Onto this mixture were added 0.1ml non-coagulated blood and various caffeine dilutions respectively. After thorough but careful mixing, the slide was immediately covered with edge-greased slip, producing air-tight condition. Petroleum jelly was used as grease. At intervals of 10mins, observations and readings were taken for an incubation period of 40 mins at room temperature. The number of sickled erythrocytes were counted and quantified in percentage. Control experiment was also done in which 0.1ml of normal saline was used in place of the caffeine solutions. Statistical Analysis: For each of the test and control experiments carried out in this work at least 9 arrays of trials were undertaken allowing for statistical analysis and correlation. Mean and Standard deviation (SD) measures of dispersion were used and student's t-test (Steel and Torrie, 1960) was used for measurement of the results significance. RESULTS In the osmotic fragility test, introduction of caffeine at its various concentrations recorded increase in lysis measured in percentage (Fig. 1). The increase in erythrocyte lysis was concentration-dependent most essentially. Lysis at 0.64% salinity (6.4g/l NaCL) was used as analytical bearing for the mean corpuscular fragility. At 0.5% salinity, the control test (0.00mM caffeine) recorded no fragility (i.e. 0.00%) while percentage fragilities of 50.0, 37.5, 24.0, 13.0, 7.0 and 1.0 were recorded at different caffeine concentrations of 10.00mM, 5.00mM, 2.50mM, 1.25mM, 0.63mM and 0.31mM respectively. The differences were highly significant (P < 0.05). Similar results were obtained at other levels of salinity. During polymerization determination (Fig. 2), the exogenous caffeine was shown to increase the polymerization of the tested haemoglobin-S, and this was also concentration dependent. For instance, at 16 mins of the observation time, there was increase in polymerized hemoglobin S by factors above the control of which from 0.625mM were significant (P<0.05). In addition, characteristic graphical shapes exhibiting a long phase followed by a partial plateau phase was observed. The effect of caffeine on sickling rate (Fig 3) showed increase in the HbS erythrocyte rate of sickling which was still concentration dependent. At the 20 mins critical value of analysis, there were varying percentages of sickling with various dilutions of caffeine. At this half time of incubation, 10mM produced the most remarkable value of 74.39% (while 0.625 mM gave 30.42% (compared to the control of 22.62% (showing percentage differences in high significance (p < 0.05). DISCUSSION From the results obtained, it was observed that the presence of caffeine at varying concentrations in blood produced increment in all the three criteria on which the experiments were based in vitro thus by extrapolation a possible physiologic significance of pro-sickling action in vitro. Indeed, this magnified some intricate consequences and properties of caffeine within the prevailing experimental conditions in contrast to some anti-sickling agents, specifically the uric acid (Ekeke and Nsirim, 1987) and urea which were constituted principally of purine ring and a metabolite of purine nucleotide metabolism respectively. The increase in polymerization of haemoglobin-S observed with exogenous caffeine possibly implies some physiologic modulation of caffeine. This might be direct or otherwise, on the concentration of the deoxyhemoglobin S and its molecules thus producing deoxyhemoglobin-S solutions of solubility less than 16 g/dl of pure deoxyhemoglobin-S solution at physiologic condition (Ross et al 1977). Furthermore, caffeine probably is prosickling also by its interaction and easy passage through biological membranes (Von-Bosstel, 1983) of which erythrocyte membrane is one. This is demonstrated by the increase in osmotic fragility of the HbS erythrocytes, an observation which relates to metabolic alteration of some ions and thus the possibility that exogenous caffeine increases the intracellular concentration of sodium and calcium ions, and possible changes in ATP level (Eaton et al, 1976, Clark et al, 1978, Clark et al 1981). Similarly, some increase was observed for sickling rate of HbS erythrocytes with exogenous caffeine. In fact, this demonstration suggested that the results observed with both criteria above were really a reflection and supportive of caffeine actions in SCD subjects. Therefore, in producing or processing any product, mostly foods and drugs containing caffeine as an additive, - principal ingredient or as a therapeutic constituent - the concentration inherent would be a critical factor most essentially for the SCD subjects. Though, there is no concise information available in literature on caffeine content of foods and drugs in Nigeria, an adaptation (Harold, 1992) showed that based on this work, most instant coffees, cola drinks and caffeine-containing analgesics (54 mg in 180 ml, about 35.5mg in 360ml and 31.63mg per 500mg tablet respectively) consumed would be experienced to enhance much sickling process in SCD subjects. And by a higher degree by foods and special drugs containing higher concentration of caffeine. Therefore, consumption of these foods and drugs by SCD subjects during crisis certainly would aggravate the condition. However, if this in vitro ation could be reproducible in vitro, by implication, eschewing caffeine containing foods, replacing caffeine containing special drugs during sickle cell crisis would play a major role in the process of SCD subjects recovery. ACKNOWLEDGEMENT The staff of Department of Haematology (Laboratory) UPTH, Port Harcourt are thanked for assistance during this research. REFERENCES
Copyright 2002 - Journal of Applied Sciences & Environmental Management The following images related to this document are available:Photo images[ja02015f1.jpg] [ja02015f2.jpg] [ja02015f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}