 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
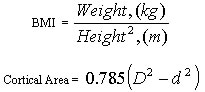
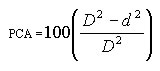
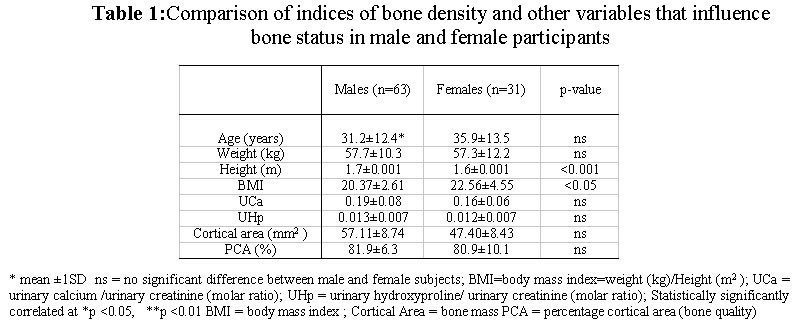
Journal of Applied Sciences & Environmental Management, Vol. 7, No. 1, June, 2003, pp. 19-23 Urinary and Anthropometrical Indices of Bone Density in Healthy Nigerian Adults George, B O Department of Biochemistry, Delta State University, Abraka, Nigeria, E-mail ebelegeorge@yahoo.com Code Number: ja03004 ABSTRACT: Measurements on the x-ray of the 2nd metacarpal of the right hand and 2h fasting urine sample were used in a cross sectional study to assess urinary indices of bone density (bone mass, percentage cortical area, PCA) in 94 healthy Nigerian adults aged between 19-72 years. Body mass index (BMI) was also estimated. No significant gender - difference was observed in most of the parameters with exception of bone mass, which was larger in the males (57.11± 8.74 mm2 and 47.40±8.43 mm2 for males and females respectively, p < 0.05) and BMI, which was higher in the females (20.37± 2.61 and 22.56 ± 4.55, for the males and females respectively (p < 0.05). In both groups there was a significant association between urinary hydroxyproline and urinary calcium (r = 0.845, p < 0.001, and r = 0.412, p < 0.001) for females and males respectively. Urinary calcium and hydroxyproline was associated with age in the female (r = 0.530, p < 0.001) only. Bone mass correlated with urinary calcium in the males (r = -0.356, p < 0.05), while urinary hydroxyproline was inversely associated with PCA in the female group. Stepwise multiple regression analyses revealed that in this study, the best urinary and anthropometric determinants of bone mass were urinary calcium and height in the males, and weight and age in the females. Furthermore, urinary hydroxyproline was the best predictor of PCA in both male and female subjects. The relationships observed between BMI, age, urinary hydroxyproline, urinary calcium, and bone density indices suggest that these variables can be used to monitor or assess bone status in healthy individuals. @JASEM The bone is a connective tissue that provides a mechanical support for the body protects vital organs and in addition serves as a metabolic reservoir of calcium and phosphate in the body (Parfitt, 1983), because 99% of the body calcium and 85% of phosphorus are found in the skeleton. The adult bone is a dynamic tissue constantly being formed and resorbed. If formation does not keep pace with bone resorption the bone becomes porous, progressively more brittle and fragile. Bone loss is synonymous with loss of calcium from the body and changes in bone metabolism have been measured using urinary calcium and hydroxyproline levels. In addition, urinary hydroxyproline levels have been considered as an index of bone resorption and a major determinant of bone status (Nordin et al., 1986; Gotfredsen et al., 2001). Other simple measurable predictors of bone mass such as weight, height and body mass index (BMI) have also been used (Smerdely et al., 2000). Bone density has been assessed by measuring cortical thickness of the second metacarpal as an index of bone mass (Wishart et al., 1993), while percentage cortical area (PCA) has also been used to assess bone quality (Garn et al 1981). The bone status of an individual or community includes not only the present bone size but also the direction in which it is likely to move. There is limited information on urinary excretion of calcium and hydroxyproline in relation to bone density among Nigerians. Moreover, there is the possibility of asymptomatic bone loss among Nigerians that could compromise an individual's bone status since loss of height, a component of osteoporosis, has been observed among elderly Nigerian females (George et al., 2000). A cross sectional study of Nigerian adults has therefore been undertaken to assess urinary determinants of bone density (bone mass, and PCA). In addition, monitoring bone status through urinary excretion of calcium and hydroxyproline could serve as a surveillance measure in early intervention against excessive bone loss whether due to age, or malnutrition. Assessing bone mass by measuring cortical thickness or bone turnover through measurement of urinary hydroxyproline or calcium could form tools available to assist health care professionals in predicting those at risk of excessive bone loss. This paper reports on the urinary calcium and hydroxyproline levels as well as height, weight and BMI in relation to indices of bone density in healthy adults. MATERIALS AND METHODS The study group consisted of 94 volunteers (31 females and 63 males) aged 19-72 years. Participants were free-living non-smokers, and ambulatory. The women were neither pregnant nor on oral contraceptives and were not undergoing menstruation during the study period. None of the participants had suffered any fracture in the previous two years, nor were they on any medication that might affect calcium metabolism. The Oyo State Health Council approved the study, and informed consent was obtained from each participant. Posterior-anterior X-ray film of the right hand was taken. Bone density was estimated by calculating cortical area (CA) and percentage cortical area (PCA) at the midshaft of the second metacarpal using the formulae:
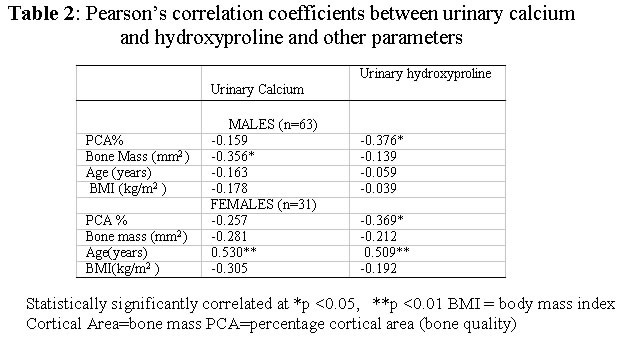
where D is the outer diameter, and d the medullary cavity diameter (Garn et al 1971). The index PCA represents the proportion of the cross-sectional area that is composed of cortical bone and has been used as a measure of bone quality (Garn et al., 1981). Cortical area is an indicator of bone. The measurements were made to the nearest 0.01mm with a vernier rule. Thus in this study PCA and bone mass are used as indices of bone density. A 2-hr fasting urine sample was collected from each participant. The urine was discharged into clean plastic bowls containing 1ml of concentrated hydrochloric acid added as a preservative. After thorough mixing by swirling the contents, aliquot samples were taken into smaller clean plastic bottles and kept frozen at -20°C until analysed. Urinary creatinine was determined according to Howells and Whitehead, (1967). Urinary calcium (Trudeaux and Freier 1974) as well as hydroxyproline (Kivirikko et al., 1967) were also determination. The urinary calcium is expressed as urinary calcium to creatinine ratio by dividing the calcium concentration in mmoles per litre by the creatinine concentration in mmoles per litre. Similarly hydroxyproline is also expressed as hydroxyproline to creatinine ratio. The differences between the means of the various parameters were compared using student's t-test, while urinary and anthropometric predictors of bone density were sort using stepwise multiple regression analysis. Associations among the parameters were also determined by calculating Pearson's correlation coefficients. These statistical analyses were performed using SPSS for Windows (version 9.0), and were considered significant at p-values < 0.05. RESULTS AND DISCUSSION Calcium salts in bone are embedded in collagen fibrils 13% of which are mainly hydroxyproline. During bone loss, collagen fibrils are broken down and hydroxyproline is excreted in the urine. Urinary hydroxyproline is thus considered as an index of bone resorption (Nordin et al., 1986). Urinary calcium and hydroxyproline are expressed in relation to creatinine in this study because creatinine is excreted in the urine as creatinine phosphate in relatively constant amounts proportional to an individual's muscle mass (Heymsfield et al., 1983) thus serving as a reference standard. Since only 3% of the total hydroxyproline found in the urine is free, the remainder is bound to small peptides. For this reason, urine samples for total hydroxyproline analysis are first hydrolysed. However, the hydrolysate would contain pigments, which interfere with the chloroamine T used as chromophore. The method of Kivirikko et al., (1967) permits the removal of the pigments by centrifugation before the pyrrole is extracted into toluene and its concentration determined. Investigators have shown that the excretion of hydroxyproline in random samples reflected the excretion in levels obtained in 24-hour samples (Matsuki et al., 1982). It has also been shown that calcium, phosphate and hydroxyproline excretion in 2-hour fasting urine sample in relation to creatinine of both normal and osteoporotic subjects, compared favourably with values from 24-hour sample (Sebert et al., 1981). Thus, the values obtained from the urine samples in this study represent calcium coming from the bone. In Table 1, bone density indices and urinary and other parameters that influence these indices are compared in male and female subjects. With the exception of bone mass, which was significantly greater in the males (p < 0.001) and body mass index (BMI), which was significantly higher in the females (p < 0.05), there was no gender difference in the variables measured. Table 2 presents Pearson's correlation coefficients showing the extent to which urinary hydroxyproline and calcium were associated with the other variables used in this study. In the female subjects, urinary calcium and hydroxyproline excretion increased significantly with age (r =0.530 and r = 0.509, p < 0.01 respectively). Although the bone mass negatively correlated with both urinary calcium and hydroxyproline levels, this correlation was not significant. However, the inverse association of hydroxyproline with PCA was significant (p < 0.05). Partial correlation analysis showed that this correlation was dependent on BMI ( r12.3 = -0.340, p > 0.05), in the females. The data also showed a significant inverse association between hydroxyproline and PCA (r = -0.376, p < 0.05) among the males and a negative correlation between urinary calcium and bone mass that was not dependent on BMI (r = -0.356 p < 0.001,r12.3 - 0.362, p < 0.05). There was also a significant correlation between urinary calcium with hydroxyproline level in both the male and female subjects (r = 0.412, p < 0.02, and r = 0.845, p < 0.001 in males and females respectively). These relationships were not influenced by age. The analysis also revealed that the best determinants of urinary calcium in the subjects after hydroxyproline was age in the females (r = 0.530, p < 0.001) and bone mass in the males(r = -0.356 p < 0.005). It may be inferred from the association between urinary calcium and hydroxyproline that factors affecting calcium excretion would also promote hydroxyproline excretion. Indeed, high urinary sodium and phosphorus (Goulding et al., 1986) excretion have been reported to be associated with increased urinary calcium excretion. Thus the general advice would be to reduce the intake of foods and beverages that contain high levels of sodium and phosphorus should be reduced in order to guard against excessive rate of bone resorption. In addition, the relationship between PCA and age in the females was dependent on urinary calcium and hydroxyproline levels. The inference from this data could therefore be that during the period of aging when calcium absorption (Alvioli, 1980) as well as bone density was decreasing, calcium loss (as a measure of bone resorption ) becomes a crucial factor on bone status measurement in this group. Results from this study also showed that the BMI in the women was associated to bone mass (r = 0.371, p < 0.05), this could be in agreement with the reported positive relationship between the fraction of absorbed calcium with BMI in menopausal females, that accounted for a substantial proportion of variance in bone density in females (Devine et al.,1993). In this study, multiple linear regression analysis was also carried out to identify variables significantly related to these indices of bone density. The results showed that, in the females weight and age were the best predictors of bone mass, while urinary hydroxyproline was the best predictor of PCA. In the male volunteers however, height and urinary calcium, were best predictors of bone mass, while urinary hydroxyproline was best for PCA. As already stated, the bone status of an individual or community includes not only the present bone size, but also the direction in which it is likely to move. Methods such radiogrammetry (Wishart et al., 1993), and photon absorptiometry (Chowdhury et al., 2001) have been used, for in vivo measurements. Recent studies have shown a sustained interest in the importance of maximizing peak skeletal mass (PSM) (Kun et al., 2001) and the importance of monitoring bone loss. The bone mass of an individual especially at menopause or at the onset of age-related bone loss, is considered as the difference between PSM reached at adulthood and bone lost through ageing thus the skeletal size before the onset of bone loss becomes an important determinant of bone mass at menopause as well as the occurrence of osteoporosis and subsequent resistance to fractures. It has been shown that adequate calcium intake by children and adolescent is important to achieving PSM (Kun et al., 2001). The results from this study suggests that indices such as urinary calcium and hydroxyproline as well as age and BMI could be used as simple indicators to monitor or evaluate the direction of bone development to enable early intervention so as to minimize fractures that could be due to either age-related bone loss, or malnutrition. There is therefore the need to establish normal acceptable ranges for urinary excretion of calcium and hydroxyproline in various communities beyond which individuals could be at risk of excessive bone loss and consequently be predisposed to fractures. In addition, the efficacy of calcium supplementation in clinical trials could be evaluated by monitoring urinary calcium and hydroxyproline levels. In this study, the results suggests that the effect of age on bone mass seems to be more important in females than in males in addition the significant correlation between urinary hydroxyproline and urinary calcium suggest that factors that could increases the excretion of urinary hydroxyproline would affect the quality of bones in both male and female subjects. It has recently been reported that, although age, BMI, urinary calcium and hydroxyproline were among the variables that affected bone density hydroxyproline and osteocalcin were determinants of femoral bone mineral density in healthy men, testosterone cortisol and BMI were more significant determinants for lumber spine BMD in the same individuals (Celtin et al., 2001). It thus appears then that, the determinants of bone status in general depended on the type of bone indices used, and the gender of the study group. If preventive measures are to be initiated prior to the onset of excessive bone loss, they may be considered early by monitoring bone density using simple non-invasive indicators. Assessing bone mass by measuring cortical thickness or bone turnover through measurement of urinary hydroxyproline or calcium could form tools available to assist health care professionals in predicting those at risk of excessive bone loss. Concluding, the results of this study suggest a relationship between BMI, age, urinary hydroxyproline, urinary calcium, and bone density. These parameters are easy, non-invasive, analytes that can therefore be used to monitor or manage age-related bone loss or increased bone loss due to metabolic bone disease or malnutrition. ACKNOWLEDGEMENTS The author appreciates the cooperation, of the participants and the assistance rendered by the medical staff of Igbo-Ora Rural Health centre and Erua District Hospital, most especially Mrs Awojobi now of Awojobi Clinic Erua for X-ray facilities and the Oyo State Health Council for approving the study. REFERENCES
Copyright 2003 - Journal of Applied Sciences & Environmental Management The following images related to this document are available:Photo images[ja03004t1.jpg] [ja03004t2.jpg] |
| |||||||||
{kind=link}
{kind=link}