 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
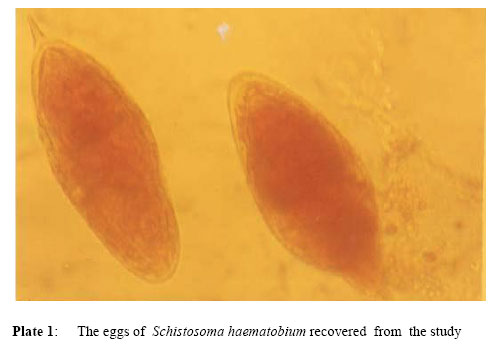
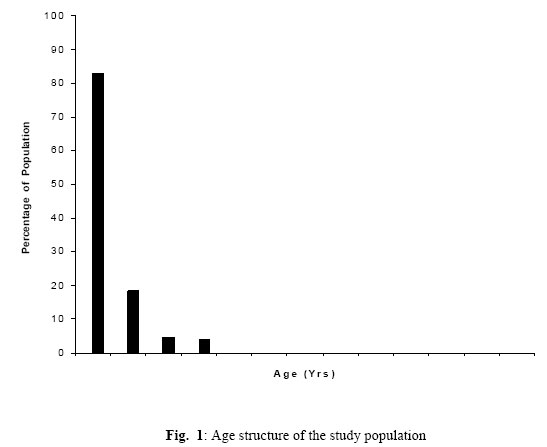
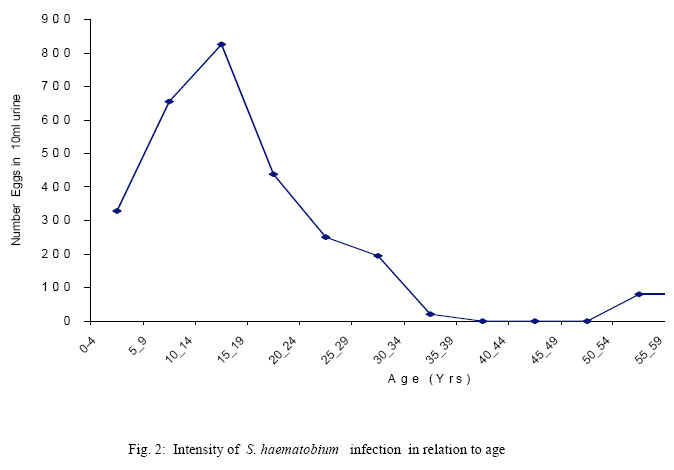
Journal of Applied Sciences & Environmental Management, Vol. 9, No. 3, 2005, pp. 37-43 The Epidemiology of Schistosoma haematobium in Odau Community in the Niger Delta Area of Nigeria *AGI, P I; OKAFOR, E J Department of Animal and Environmental Biology, Faculty of Science, University of Port Harcourt, Nigeria Code Number: ja05056 ABSTRACT: A study was conducted between August 2001 and July 2002 to investigate the current pattern of prevalence and intensity of Schistosoma haematobium infection at Odau Community in the Niger Delta Area of Nigeria.. Three hundred urine specimens were examined from randomly sampled individuals aged between 0 years and 73 years. More than 50% of the participants were under the age of 20 years, and the population sampled had a male to female ratio of 37:23. Quantitative microscopic counting of Schistosoma haematobium eggs was carried out. Two hundred and fifty participants out of the three hundred examined were positive for the infection, representing an overall estimated prevalence of 83.3%. The infection rate peaked (93.0%) in the 10-14 years age category. A significant negative correlation (r =0.306, P < 0.1) was found between age and intensity of infection. The age and sex pattern of Schistosoma haematobium infection as obtained from the study area showed a typical peak prevalence in early adolescence with males having a higher prevalence rate (84.9%) than females’ (80.9%) (χ2 = P > 0.01). The high rates of prevalence and intensity of Schistosoma haematobium observed in the present study clearly indicated that Odau Community is facing a great health burden especially the children and women who had severe infections. @JASEM Schistosomiasis is a wide spread parasitic infection caused by blood flukes of the genus Schistosoma and transmitted by specific fresh water snails. The infection is reported to have plagued the humans since the ancient times (El-Harvey et al; 2000). Some of the factors which influence the transmission of schistosomiasis in an endemic area include the presence of snail intermediate hosts of the parasites and human contact with the infected waters. Out of the three main human infecting species of Schistosoma (S. haematobium, S. mansoni and S. japonicum), S. haematobium is the predominant species in Africa being endemic in about 53 countries in Africa and the Middle East (Ejezie, 1991; Ogbe, 1995). Urinary schistosomiasis, caused by S. haematobium is noted to be more prevalent in Nigeria than intestinal schistosomiasis due to the wider distribution of its snail host Bulinus species (Ejeizie, 1991; Ugbomoiko, 2000) This is in addition to indiscriminate passing of urine containing S. haematobium eggs into water supplies containing the snail host (Southgate and Rollinson, 1987). Records of prevalence and intensity of urinary schistosomiasis in areas of endemicity show an infection pattern which seems to peak in individuals in their first two decades of life, and with varing rates (Ogbe, 1995, El-Harvey et al; 2000). When compared with their adult counterpart, children with schistosomiasis notedly harbour greater worm burden and are more intensely infected due to the high transmission rates of the parasite and the frequency of exposure to infection sites (Ogbe, 1995). Individuals who are encountering the infection for the first time may exhibit severe infections irrespective of their age and sex. In countries with a long history of schistosomiasis research studies have identified the risk factors for infection with S. haematobium as male gender, an age < 20 years, living in smaller rural communities, exposure to canal waters, reagent strip detected haematuria and proteinuria, and a history of burning micturition (El-Harvey et al; 2000; Abdel-Wahab et al; 2000; Gabr et al; 2000). The amount of eggs excreted and quantified in 10ml of urine specimen expresses the intensity which may be associated with the severity of the internal damage (Loverde and Chen, 1991). In S. haematobium endemic area evidence has shown that long term infections are associated with certain risks of urinary involvement which manifest as haematuria, proteinuria, pathology of the urinary tract, iron deficiency anemia and impaired growth (Warren et al; 1979; Stephenson et al; 1985; Belidi-Mengue et al; 1992; Abdel-Wahab et al; 2000). Severity of the disease may result to bladder cancer later in adulthood (Mustafa et al; 1995) There are continuous increase in the prevalence and intensity of urinary schistosomiasis in many endemic communities in Nigeria (Anosike et al; 1999). S. haematobium infection has been found endemic in Rivers State (Agi, 1995). Few foci of S. mattheei and S. intercalatum have been noted by Arene et al; 1989). The world Health Organization (1985) has recommended that the combined use of antischistosomal drugs with environmental sanitation and health education could drastically reduce the prevalence and intensity of S. haematobium. This method of control has been used for schistosomiasis in some endemic areas with desirable results (Doenhoff et al; 2000; Habib et al;2000). The present study examines the current pattern of prevalence and intensity of S. haematobium infection at Odau community in the Niger Delta Area of Nigeria. MATERIALS AND METHODS Study Area: The study was conducted in Odau, a rural community in Niger Delta Area of Nigeria made up of mainly peasant farmers. The community is located on latitude 40° 56'N and longitude 60° 27' E, and surrounded by fresh water swamps. Most families are subsistent farmers and fresh water fisher folks. They mainly depend on various ponds and streams for their water related activities. The inhabitants of the community had neither a good road nor hospital facilities and there are no latrines, so urination and defecation are done in the bushes surrounding the village. Sample Collection: Three hundred individuals were randomly selected for the study. Participation was entirely voluntary and the people were made aware of the study and its benefits by exposing them to health education. Each participant was given a clean 40 ml universal bottle to provide terminal urine between 10.00 am and 2.00 pm. Each bottle was labelled to correspond to the number of the person’s card. Each person was sampled for two consecutive days and a duplicate 10ml urine specimen was filtered from each sample using the Nitrel filtration technique described by Mott et al (1982). Nitrel filtration equipment consists of a 10ml plastic syring, a plastic extension tube, a nilon mesh filter and filter supports. The extension tube was fitted unto the end of the syringe. The top part of the filter support was connected to the adaptor of the syringe while the bottom held the filter inside and both were tightly held together by a silicon gasket. Each urine specimen was thoroughly mixed and 10ml drawn into the syringe. The urine was forced through the filter into the filter support and the residues including schistosome eggs collected on the filter. The filter was removed from the support with a pair of forceps, placed on a clean glass microscope slide and stained with drops of Lugol’s iodine solution prior to microscopic examination. The filters were observed under a 10x objective lens of a binoculas microscope for the presence of schistosome eggs (plate 1). Few drops of water were added to the edge of the nilon mesh filter during microscopy to avoid drying up, and for easier identification of the schistosome eggs. The number of eggs obtained per 10ml of urine specimen was counted and quantified as intensity of infection. Urinalysis was carried out using Medi Test ‘Combi 9’ reagent strip capable of detecting urinary blood, protein and other parameters. The criteria for the establishment of S. haematobium infection in a given specimen were, the presence of eggs and / or positive urinalysis test. Candidates with negative biochemical and microscopic tests were used as controls. Statistical analysis was done using χ2 (chi square) tests and simple correlation coefficient r to compare differences, and for the determination of associations respectively. RESULTSThree hundred (300) urine specimens were examined. The age structure of the individuals examined is shown in Fig 1. More than 50 % of the subjects were under the age of 20 years. The rest included the adults and elderly persons. 83.3 % of the total number were infected with S.haematobium. Those who neither excreted the eggs nor were positive for the urinalysis-test accounted for the 16.7% left (Table 1). The infection level was high for all the individual age groups considered. For the candidates under 20 years, prevalence was highest (93.0 %) in the 10 – 14 year olds. There was a progressive rise in prevalence from 70% in children under 5 years to 84.2% in the 5-9 years category. A slight reduction in prevalence occurred after the peak. In the older subjects, the rate of infection was equally high, often reaching to peak level of 100% in some groups. This was however associated with their smaller sample size. However, a negative correlation (r = 0. 181; p < 0.1) occurred between age and prevalence of infection. The males had a prevalence rate of 84.9% while the females had (80.9%) (Table 1). In children of both sexes peak prevalence occurred in the 10-14 years age group with the males having a rate of 92.9% while the females had 92.8%. Sex prevalence of individuals in older age groups fluctuated between high and low values. Out of total percentage (83.3%) of people infected with S. haematobium in the community, 74.8% had eggs in their urine. Individuals in the 10-14 years age group had the highest mean egg count (825.3 eggs/10ml urine) in the survey fig 2. The lowest mean intensity (63.2 eggs/10ml urine) was obtained from members of the 60 years plus age group. No egg was obtained from subjects in the age range of 35-49 years. A significant negative correlation (r = 0.306, p < 0.1) existed between age and intensity of infection. The percentage of males excreting eggs was 64.3% while the females were 59.1%. Intensity peak in the male subjects (922 eggs/10ml urine) occurred in the 10-14 years age group. For the females, intensity peaked (985 eggs/10ml urine) in the 0-4 years age group. After age 29 years, no female was found with eggs any longer but egg excretion continued in the males up to the very later years but on very minimal rates, fig. 2. Heavy intensity (> 1000 eggs/10m/urine) occurred in 39.0% of egg excretes. 19.3% had moderate intensity (500 –1000 eggs/10ml urine), and 41.7% had light intensity (< 500 eggs/10ml urine) Individuals under 20 years had more moderate to heavy intensity than they had light intensity. 23.5% of males with positive egg count had heavy intensity against the 15.5% of the females. Generally the females were more intensely infected than the males, fig. 3. The difference was statistically significant (χ2= p <0.001). The result of urinalysis showed that haematuria occurred in 72.7% of the participants while proteinuria occurred in 82.4%, with greater frequency of occurrence in the younger age groups. Table 1: Age and sex prevalence of S. haematobium infection in the study area.
DISCUSSIONS This study has examined the prevalence pattern and intensity of Schistosoma haematobium in Odau community in the Niger Delta Area of Nigeria. The infection pattern showed a typical peak prevalence in the early adolescence with males having a higher rate. This agrees with results of similar studies in Schistosoma haematobium endemic areas (Taylor et al; 1990; Ekanem et al; 1994; Gabr et al; 2000). High prevalence rate of S. haematobium infection has been reported by some other authors in endemic areas (Pugh et al; 1980; Akokun, et al; 1994; Anosike et al; 1999). The high rate of the infection reported in the present study may be suggestive of the level of S. haematobium transmission in various foci in the community. The ponds are the main transmission foci in the community and are distributed all over the place. They provide a natural water source as well as serve as meeting point for the schistosome parasites, their intermediate host and the people. The people depend on these ponds for their fishing occupation, bathing and other domestic needs. Infection foci have also been traced to their farms. These ensure that the people continue being infected and re-infected since no intervention strategy has been carried out in the area. Individuals in their teens who are oftentimes engaged in water related activities that expose them to these infection sites run the risk of acquiring more infection and habouring more worms. As a rural remote community, the inhabitants are predominantly farmers. The adult males and females are exposed to the infection. They either contract the infection from the nearby ponds in the community or those in their farms. The higher male prevalence may have resulted from their preponderance in the survey but may not be due to over exposure to the infection sites. There are some reported cases of higher male prevalence in some endemic areas (Pugh and Gilles, 1978; Ekanem et al; 1994). Some other studies have found no significant differences in gender prevalence (Forsyth and Bradley, 1966; Wilkins, 1977). The variations in the infection pattern may be attributed to differences in geographic and environmental setting cultural and religious beliefs in each endemic area (Wilkins, 1977; Pugh & Gilles, 1978; Southgate and Rollinson, 1987). Intensity estimates were based on mean egg counts in 10ml of urine obtained from the candidates. The egg counts rose with decreasing years and reduced with increasing years thus showing a negative correction. This is in agreement with results of intensity studies in other S. haematobium endemic areas (Wilkins, 1987; El-Harvey et al; 2000; Abdel-Wahab, et al; 2000). The intensity hike in children may be attributed to increased worm burden and the high fecundity rate of the parasite, while the opposite was encountered in adult and elderly subjects who probably have reduced schistosome worms and less eggs (Ogbe, 1995). Reduced worm burden in patients of older ages may also result from the development of concomitant immunity known to occur in the infection (Woolhouse et al; 1991). The differences in the male and females intensities of infection may reflect the degree of sensitization and host response to the invading parasites as well as the extent of worm burden in the individual subject. Studies of Etim (1995), on water contact activities and schistosomiasis among women in a rural community indicated that more women than men get more severe schistosomiasis infection due to educational and economic backwardness. They may be exposed to more intense infection than their male counterparts. S. haematobium infection has reached a hyperendemic level in the community studied owning to the high rates of the infection and intensity . This shows the degree of health burden faced by the inhabitants especially the women and children who have severe infections. There is therefore the need for an urgent control of Schistosoma haematobium infection in the community, to alleviate their health problems. REFERENCES
Copyright 2005 - Journal of Applied Sciences & Environmental Management The following images related to this document are available:Photo images[ja05056f2.jpg] [ja05056p1.jpg] [ja05056f3.jpg] [ja05056f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}