 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Applied Sciences and Environmental Management, Vol. 12, No. 2, 2008, pp. 21-24 The status of Schistosoma haematobium infection in Anyu community in the Niger Delta, Nigeria. * AGI, P.I; AWI-WAADU, G. D. B. Department of Animal and Environmental Biology. University of Port Harcourt.
P.M.B. 5323. Port Harcourt, Nigeria Code Number: ja08023 ABSTRACT: A total of 3,948 urine samples were examined for schristosome infection at Anyu in the Niger Delta, Nigeria, Two thousand and forty eight (51.9%) of the people examined were infected with Schistosomiasis. Highest infection (80.4%) was recorded in the 7-10 years age group and the lowest infection occurred in the 47-50 years of age. All the age groups between 3-47 years that were examined were infected with urinary schistosomiasis. Males were more infected (55.2%) than the females (47.2%). Intensity of infection was also highest in the 4-7 years age category. About 1022 (49.9%) of the positive individuals were excreting less than 100 ova of S. heamatobium per 10cm3 of urine, while 227 (11.1%) were excreting more than 500 ova per 10cm3 of urine. Bulinus globosus was the snail vector of S heamatobium in the area. Percentage infection of the snail vector was 5.0%. Snail infection was higher during the dry season, while snail population responded to the quantity of rainfall. Based on these data, it was proposed that interception of S. heamatobuim transmission in the study area would involve mass chemotherapy and focal application of molluscicides in the community ponds during the dry season.
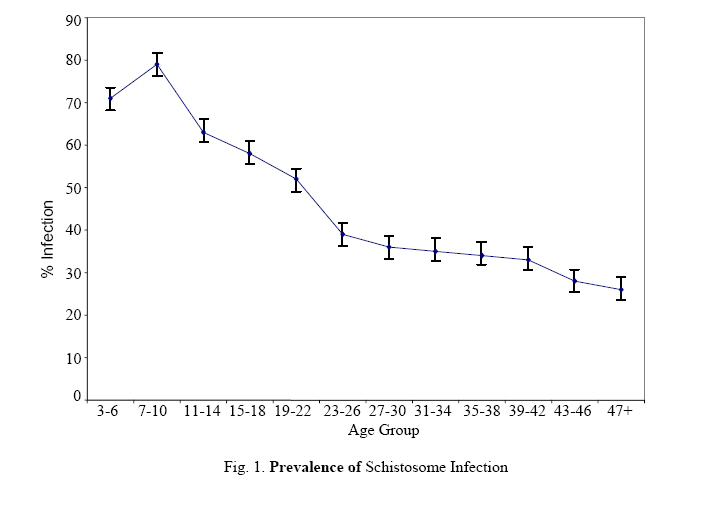
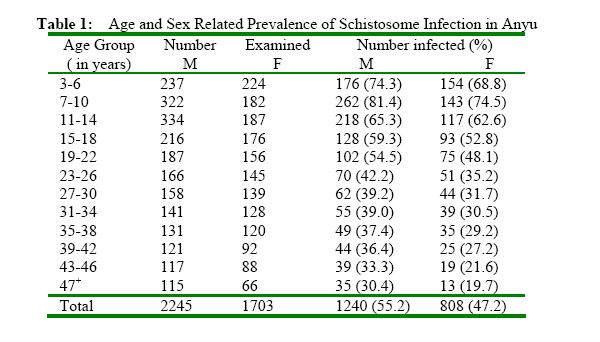
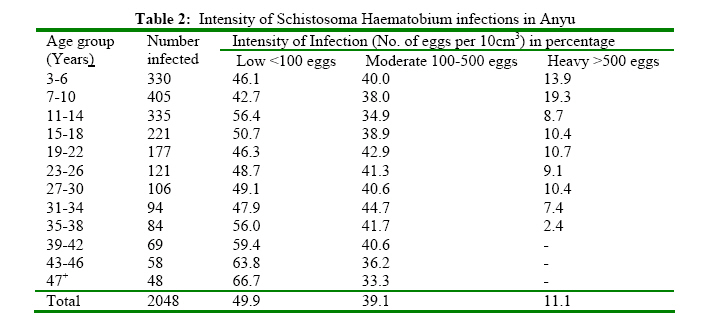
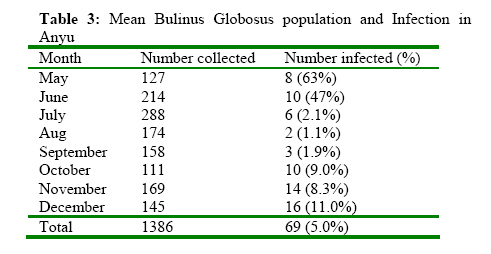
Schistosomiasis is widespread in Nigeria with a history of infection dating back to the colonial days (Blair, 1956; Cowper, 1959). Earliest studies confirmed the endemicity of the disease and the distribution of the snail vectors in the northern and western Nigeria (Cowper, 1963; Cowper, 1973) and later in eastern part (Udonsi, 1990). Subsequent studies on the morbidity indices of schistosomiasis and the dynamics of its snail vectors were carried out in these areas (Ejezie et al., 1989). Little or nothing was known about schistosomiasis in the Niger Delta until the late 1980’s (Arene et al., 1989). According to oral communication from the community, observation of haematuria began after the Nigerian civil war (1966-1969). It was thought that the Nigerian soldiers who were mainly from Northern Nigeria, brought the infection. During the first few post civil war years the infection had become widespread among primary school children in the community. Studies on the prevalence of infection and snail bionomics confirmed that Odau was hyperendemic with urinary schistosomiasis (Agi, 1995; Agi and Okafor, 2005). The extent of spread and intensity of this infection on the Southwestern axis of Orashi River, in the Niger Delta, is not known. The present study was undertaken to determine the epidemiological parameters of urinary schistosomiasis in Anyu Community in the Niger Delta, Nigeria. MATERIALS AND METHODS Study Area Anyu is situated in the high tropical freshwater swamp forest of the Niger Delta, Nigeria. Topographical and climatic characteristics of the area have been previously described (Agi, 1995). It is located on latitude 040 52’N and longitude 060 25’E. Anyu is a village with a typical rural African setting. Settlement pattern is compact and family houses are joined together. Over seventy percent of its inhabitants are poor illiterate fishermen and women. Domestic, recreational and washing water is obtained from the community ponds and two little streams which harbour a large population of Bulinus globosus, B. forskalii and Pila Ovata. There is one primary school and a newly constructed secondary school. The community has no health care center and the sick are treated at central Abua hospital, some 20km from Anyu. Collection of Urine Specimens Sample collection was preceded by an interactive meeting of the village and school heads during which period the purpose of the survey and other information relating to specimen collection were given. In schools, specimen collection was done class by class involving every student and was supervised by the class teachers who also supplied the personal data (name, age, sex, religion, source of domestic and recreational water) of each student submitting a urine specimen. Procedure for specimen collection in the village was the house-to-house approach (Udonsi, 1990). All members of the household from three years upward were requested to submit specimens. Personal data as in the previous case, including occupation, were obtained from each respondent through an interview using a local interpreter. The response received was very good because the survey was one in the series of similar studies they had in the past. Terminal urine stream was collected using tagged 30cm3 specimen bottles with screw caps. The specimens, which were collected fresh, were fixed immediately using 5 drops of 5% Formalin delivered through a pipette and carried to the parasitology laboratory in the University of Port Harcourt for analysis. Urine Examination: Each urine specimen was agitated to suspend the ova evenly. 10cm3 urine aliquot was measured into the centrifuge tube and rotated at 1500 rpm for 3 minutes. The supernant was discarded and the sediment was transferred onto a microscope slide using a micropipette (Agi, 1995). A drop of lugol’s iodine was added onto the preparation over which a coverslip was placed and examined under low and high powers of stereomicroscope. The intensity of infection was determined by counting the number of eggs in a 10cm3 aliquot of urine sample and expressed as number of eggs per 10cm3 urine. The intensity was categorized as heavy (>500 eggs / 10cm3 urine), moderate (between 100 – 500 eggs / 10 cm3 urine) or low (< 100 eggs / 10cm3 urine) (Udonsi, 1990). Snail Collection and Examination for Infection. The main water bodies (ponds, ditches and rivers) were thoroughly investigated for snail vectors of schistosomiasis using scoop nets. Routine snail survey of the water contact sites was undertaken for eight months between May and December 2003. The snail sampling techniques have been described elsewhere, the snail vectors collected were washed and examined for infection in line with the method adopted by Agi (Agi, 1995). RESULTS AND DISCUSSION A total of 3,948 urine samples were examined for the presence of the ova of S. haematobium with 2,048 (51.9%) samples positive. Peak infection (80.4%) was recorded in the 7-10 years age category. All the age groups examined were positive for S. haematobium infection. Percentage infection was high in all the age groups but gradually declined as the age increased. The lowest infection was recorded in the age group 47-50 years (fig 1). Sex related infection is shown in table 1. Overall infections in males and females were 55.2% and 47.2% respectively. Infection in the males was consistently higher in all the age groups. Peak infection in the male (81.4%) was higher but not statistically significant from peak infection (74.5%) in the female. Table 2 displays the levels of intensities. Of the 2048 infected candidates in the community, 49.9%, 39.1%, and 11.1% were excreting below 100 eggs per 10cm3 urine , between 100-500 eggs per 10cm3 urine and above 500 eggs per 10cm3 urine respectively. Consistent high intensities were recorded for candidates between 3-34 years old. Peak intensity also occurred at 7-10 years category. About 19.3% of the 405 candidates in this category were also excreting over 500-eggs/10cm3 urine. There was a decrease in heavy intensity from 31-35 years. From 39 years upwards no candidate was observed excreting more than 500 eggs per 10cm3 urine. Data on Bulinus globosus population and infection are given in table 3. Two snail species collected in the study area, capable of transmitting S. haematobium were Bulinus globosus and Bulinus forskalii. Populations of these snail vectors were high and many B. globosus were infected with S. haematobium cercariae. Infection of this snail was observed every month throughout the survey period. High snail infections, 9.0%, 8.3% and 11.0% were recorded in October, November, and December respectively, percentage infections in July (2.1%), August (1.1%) and September (1.9%) were low. Over 90% of snail population and infection occurred in the community’s fishponds and recreation ponds. It was observed that scores of children had their baths at least two times daily, before and after school in the ponds. There was no infection observed in Bulinus forskalii in the area. The study established that Anyu was a hyperendemic community for urinary schistosomiasis with high transmission foci at the community ponds near the homes. Peak prevalence occurred in the first decade of life probably because the children were infected daily by their constant contact with the infected pond water through their daily water play and recreation in the community ponds. The higher prevalence rates in the males in all the age groups were consistent with observations by other workers (Udonsi, 1990; Bassey and Uwam, 2004). The high infection rates of both genders up to the late fourth decade were unusual in the epidemiology of urinary schistosomiasis. This finding is important in the event of targetted chemotherapy. Decline in prevalence with advancing years of age was gradual probably due to decreasing human-water contacts associated with ageing (Udonsi, 1990) and senile self cure observed in Schistosoma haematobium infections (Wilkins et al., 1984; Ahmed et al., 1996)). Wiest et al (1993) noted a similar decline for S. japonicum infection but were silent about the cause. However, they observed a “progressive increase in the severity of hepatic periportal fibrosis with age, with advanced fibrosis peaking in the fifth decade”. The occurrence of infection in individuals in their late forties was attributed to the wide distribution of the infected snail vectors and the frequency of human water contact. The heavy schistosome infections in all the age groups were a result of close proximity of homes to the transmission foci (ponds) which were the only source of domestic, washing and recreational water (Arene et al., 1989). Intensity of infection was related to prevalence. This observation has been noted by some researchers (Udonsi, 1990; Ejezie et al., 1989; Agi, 1995). A large proportion of the infection was in the “low intensity” category suggesting that the community was dynamic. The absence of heavy intensity beyond 38 years of age could be explained by the possible role of protective immunity (Wilkins et al., 1989). Bulinus globosus has been incriminated as a vector of Schistosoma haematobium (Ejezie et al., 1989; Arene et al., 1989) while snail population increased with the volume of rainfall, snail infection was higher in the drier months. The reduction of snail population between July and September was attributed to the annual flooding of the entire community which swept large numbers of snails. This was responsible for the low percentage snail infection during the period. There was no infection observed in B forskalii in the area. Elsewhere B forskalii is involved in S. intercalatium transmission (Arene et al., 1989; Chuem and Jourdane, 1993). Knowledge of these base-line epidemiological parameters is important in planning and executing Schistosome control programmes in the study area. REFERENCES
Copyright 2008 - Journal of Applied Science and Environmental Management The following images related to this document are available:Photo images[ja08023t1.jpg] [ja08023t2.jpg] [ja08023t3.jpg] [ja08023f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}