 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Comparative Study of Erythrocyte Sedimentation Rate (ESR) Using Trisodium Citrate, Normal Saline and Whole Blood in Ethylene Di Amine Tetra Acetic Acid (EDTA) 1Emelike, O.F.; 1Akpan, J.E. 1Obigwe, B.U.; 2*Jeremiah, Z.A.1Department of Haematology, Faculty of Basic Medical Sciences, College of Medicine, Ambrose Alli University, Ekpoma, Edo State-Nigeria.
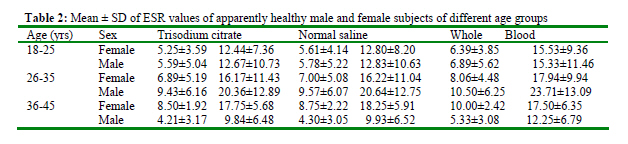
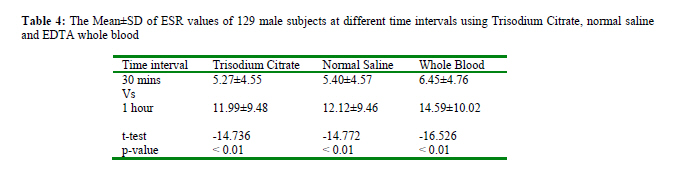
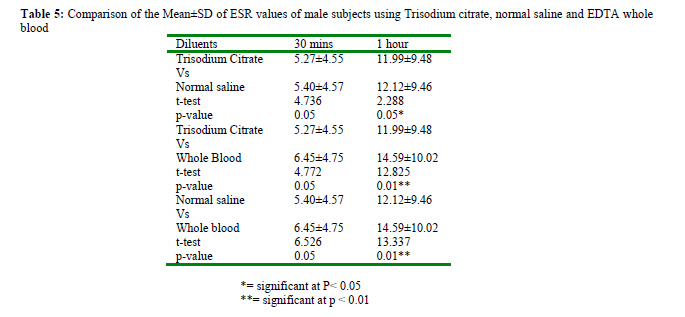
Code Number: ja10004 ABSTRACT Erythrocyte sedimentation rate (ESR) was carried out on 200 apparently healthy individuals (131 males and 69 females) in Ekpoma using trisodium citrate, normal saline diluents and whole blood suspension in EDTA without any diluents. The Westergren method was adopted for this study as recommended by the International Committee for Standardization in Haematology (ICSH). The tests were read at 30 minutes and 1 hour intervals and results recorded as mm in 30mins and mm in 1hr respectively. The Mean ± SD of ESR values in males using trisodium citrate and normal saline were 11.99±9.48 and 12.12±9.46, while for females it was 13.69±8.5 and 13.97±8.97 respectively. This difference was statistically significant (P< 0.05). There was also a statistically significant difference between the ESR values obtained using trisodium citrate and whole blood (P< 0.05). Males had lower ESR values compared to females. There was a statistically significant difference between the ESR values obtained in 30mins and 1 hour (P< 0.05). In conclusion, the use of normal saline and whole blood cannot be a good substitute for trisodium citrate in estimating ESR. Secondly, ESR is time dependent; therefore, the conventional time of 1 hour should be maintained. @ JASEM Blood is a living tissue which consist of a straw coloured fluid medium called plasma in which red blood cells (erythrocytes), white blood cell (leukocyte) and platelets(thrombocytes) are suspended (Baker et al., 2001 ). The main function of the circulating blood is to carry oxygen and other nutrients through the body and to remove carbon dioxide and waste products, provides an efficient defence against infection and maintain the integrity of the circulating system (Hall and Malia, 1998). It has physiochemical properties such as isotonicity, colloid osmotic pressure and viscosity as characteristics, rheological properties influenced by the rouleaux formation of erythrocyte all of which collectively permit circulation and formation of the blood constituent (Hall and Malia, 1998).Erythrocyte sedimentation rate (ESR) also called the Sed rate determination is a simple, inexpensive non-specific laboratory test that is frequently ordered in clinical medicine. The test measures the distance erythrocytes fall after an hour in a vertical column of anticoagulated blood under the influence of gravity (Saadeh, 1998). The basic factors influencing the ESR have been understood since the early part of this century; the amount of fibrinogen in the blood directly correlates with the ESR (Wetteland et al., 1996). There are two main methods of performing the ESR; the Wintrobe and Westergren method (Lewis et al., 2006). The most satisfactory method of performing the test was introduced by Westergren in 1921 and recommended by the International Council on Standardization in Haematology (ICSH) (Emeribe and Ukonu 1992). ESR helps in the diagnosis of those conditions associated with acute and chronic inflammation, including infections, cancers, and autoimmune diseases. ESR is said to be non-specific because its increase do not tell exactly where the inflammation or what is causing it, and also because it can be affected by other conditions besides inflammation. For this reason, ESR is typically used in conjunction with other tests (Saadeh, 1998). The test is best carried out within two hours of blood collection although a delay of up to 6 hours is permissible provided that the blood is kept at 4oC (Emeribe and Ukonu, 1992). The ESR is governed by the balance between prosedimentation factors, mainly fibrinogen, and those factors resisting sedimentation, namely the negative charge of the erythrocytes (zeta potential) (Bridgen, 1999). When an inflammatory process is present, the high proportion of fibrinogen in the blood causes red blood cells to stick to each other. The red cells form stacks called 'rouleaux' which settle faster. Rouleaux formation can also occur in association with some lymphoproliferative disorders in which one or more immunoglobulins are secreted in high amounts (Bridgen, 1999). Although it is frequently ordered but the erythrocyte sedimentation rate (ESR) is of limited use as a screening test in symptomatic patients. It is useful for diagnosing diseases, such as multiple myeloma, temporal arteritis, polymyalgia rheumatica, various auto-immune diseases, systemic lupus erythematosus, rheumatoid arthritis, and chronic kidney diseases (Wise et al., 1991). In many of these cases, ESR may exceed 100 mm/hour. It is commonly used for a differential diagnosis for Kawasaki's disease and it may be increased in some chronic infective conditions like tuberculosis and infective endocarditis. It is an index for the assessment of severity of inflammatory bowel disease in children (Mack et al., 2007). The clinical usefulness of erythrocyte sedimentation rate (ESR) is limited to monitoring the response to therapy in certain inflammatory diseases such as temporal arteritis, polymyalgia rheumatica and rheumatoid arthritis. It can also be used as a crude measure of response in Hodgkin's lymphoma (Wolfe, 1994). Additionally, ESR levels are used to define one of the several possible adverse prognostic factors in the staging of Hodgkin's lymphoma (Wolfe, 1994). Trisodium citrate is almost exclusively used as the diluent of choice for setting up ESR, but some contemporary laboratories have resolved to use normal saline as the diluent of choice while others set ESR using whole blood without any diluent. However, this study is geared towards analyzing the relationship between these diluents in order to establish an acceptable method that may be cheaper but yield a reliable result. This study was therefore designed to determine the relationship between using trisodium citrate, normal saline and whole blood to set ESR, hence source for a cheaper alternative, relationship between males and females values of ESR and effect of time (30 minutes and 60 minutes) of ESR MATERIALS AND METHODS Study area and Subjects: This study was carried out in Ekpoma, Esan West Local Government Area, Edo state. Ekpoma is fairly an urban area with a State University situated in it. It is located at Latitude 6.75oN and Longitude 6.13oE with a population of 61,870 (Population of cities, 2007). A total of 200 apparently healthy subjects were recruited for this study (131 males and 69 females), within the age range of 18 - 50 years. The subjects comprised of students of Ambrose Alli University, Ekpoma and indigenes of Ekpoma. Five milliliters of venous blood was collected from each subject with the aid of a sterile disposable needle and syringe and expressed into appropriately labelled ethylenediaminetetracetic acid (EDTA) specimen container and the specimens were used within two hours of collection. Method: Westergren (Lewis et al., 2006): When citrated blood in a vertically positioned westergren pipette is left undisturbed, red cells aggregate, stack together to form rouleaux, and sediment through the plasma. The ESR is the rate at which this sedimentation occurs in one hour as indicated by the length of the column of clear plasma above the red cells measured in "mm" (Lewis et al., 2006). 0.4millilitre of trisodium citrate and 0.4millilitre of normal saline was pipetted into two different test tubes. 1.6millilitre of EDTA anticoagulated blood was added to the two tubes and 2millilitres of blood was added to a third tube. The mixtures were properly mixed and used to set ESR with disposable ESR tubes. After 30 minutes and 1 hour, the results of the sedimentation was read and recorded appropriately in mm per hour Statistical analysis: Mean, standard deviation and student t-test at 95% confidence limit were used to analyse the results obtained. RESULTSTable 1 summarizes the mean±SD of the ESR values of apparently healthy male and female subjects in Ekpoma using trisodium citrate, normal saline and whole blood at 30 minutes and 1 hour. The results showed that of the 200 subjects tested, 129 were males and 69 were females. The mean±SD of the ESR values of males at 30 minutes using trisodium citrate, normal saline and whole blood were 5.20±4.55, 5.40±4.57 and 6.45±4.76 respectively. While for females, it was 5.85±4.06, 6.14±4.36 and 7.01±3.87 respectively. At 1 hour, the ESR values for males were for trisodium citrate, 11.99±9.48, Normal saline 12.2±0±9.46 and whole EDTA blood, 14.89±10.02 mm/hr. Table 2 Shows the Mean±SD of the ESR of 12.25±6.79 respectively. The mean±SD of the ESR apparently healthy males and females of different age of males within the age of 26-35 years at 30 minutes groups. The mean+SD of the ESR of males within using trisodium citrate, normal saline and whole the age of 18-25 years at 30 minutes using trisodium blood was 5.59±5.04, 5.78±5.22 and 6.89±5.62 citrate, normal saline and whole blood was respectively. At 1 hour, the mean±SD of ESR values 4.21±3.17, 4.30±3.05 and 5.33±3.08 respectively. for males using trisodium citrate, normal saline and While for females it was 5.25±3.59, 5.61+±4.14 and whole blood was 12.67±10.73, 12.83±10.63 and 6.39±3.58 respectively. At 1 hour the ESR values for 15.33±11.46 respectively. For female subjects, the males using trisodium citrate, normal saline and ESR values at 30 minutes was 6.89±5.19, 7.00±5.08 whole blood was 9.84±6.48, 9.93±6.52 and and 8.06±4.48 respectively. ESR values for females at 1 hour using trisodium citrate, normal saline and whole blood was 16.17±11.43, 16.22±11.04 and 17.94±9.94 respectively. The ESR values for male subjects within the age of 36-45 years at 30 minutes using trisodium citrate, normal saline and whole blood was 9.45±6.16, 9.57±6.07 and 10.50±6.02 respectively. At 1 hour, the ESR values for males using trisodium citrate, normal saline and whole blood was 20.36±12.89, 20.64±12.75 and 23.71±13.09 respectively. The ESR values for female subjects at 30 minutes using trisodium citrate, normal saline and whole blood was 8.05±1.92, 8.75±2.22 and 10.00±2.45 respectively. At 1 hour, the ESR values for females using trisodium citrate, normal saline and whole blood were 17.75±5.68, 18.25±5.91 and 17.50±6.35 respectively. Table 3 shows the comparison of the mean+SD of the ESR values of apparently healthy males and females (effect of sex) in Ekpoma using trisodium citrate, normal saline and whole blood at 30 minutes and 1 hour. The comparison showed a significant difference (p< 0.05). Table 4 Shows the Comparison of the mean±SD of ESR values of the subjects at different time intervals using trisodium citrate, normal saline and whole blood. Table 5 Shows the Comparison of the mean±SD of ESR values of male subjects using trisodium citrate, normal saline and whole blood for trisodium citrate vs normal saline, trisodium citrate vs whole blood and normal saline vs whole blood. There was a marked significant difference between 30 minutes and 1 hour, (P< 0.01) DISCUSSION This study was aimed at analyzing the relationship between setting up ESR with trisodium citrate, normal saline and whole blood in order to establish an acceptable method that may be cheaper but yield a reliable result. A comparison of ESR results obtained using the conventional diluent, trisodium citrate with those obtained with normal saline as diluent showed a significant difference between the two diluents for males and females. This observation is not in agreement with an earlier report by (Emeribe and Ukonu, 1992) who stated that there is no significant difference in trisodium citrate and normal saline. Setting ESR using whole blood showed a significant difference, as the values obtained was higher than trisodium citrate and normal saline respectively. The reason for this observation is not immediately known. It may however be that trisodium citrate reduces rouleaux formation than whole blood leading to increase ESR in whole blood or it might be a difference in viscosity, where whole blood may be less viscous than trisodium citrate resulting to higher values. ESR values of whole blood were significantly higher than trisodium citrate. This therefore, disqualifies the use of normal saline and whole blood to set up ESR in the contemporary medical laboratory. Females had higher ESR values than males which agree with earlier report by (Saadeh, 1998). The reason for this increase may be due to some physiological changes that occur in females like menstruation. References ESR values for male and female residence in Ekpoma was 11.99+9.48mm and 13.69+8.59mm respectively for the first hour. This was significantly higher than text book values reported for Caucasians. This may be because of climatic differences (e.g. higher ambient temperature) or higher level of serum globulin due to endemic Parasitaemia in the tropics (Emeribe and Ukonu, 1992; Gillium, 1993). The room temperature at the time of this study was between 27oC - 30oC as compared with 18oC- 25oC under which most Caucasian values were obtained. Temperature varies directly with ESR (Hall and Malia, 1984). Serum globulin and other macromolecular proteins increases rouleaux formation and hence the sedimentation rate (Viroj, 2008). The difference between the ESR values at 30 minutes and 1hour of test was significant. This agrees with an earlier report by (Emeribe and Ukonu, 1992) who stated that there was a significant difference in ESR values at 30 minutes and 1 hour. This study confirms that reading the test at the conventional time of 60 minutes should be strictly followed. It is however concluded that the use of normal saline and whole blood in place of trisodium citrate should be disregarded. CONCLUSION We concluded that trisodium citrate is the best diluent to be used in the contemporary laboratory to set ESR. This study also raised a reference value of 11.99+9.48mm and 13.69+8.59mm for males and females respectively resident in Ekpoma. ESR increases with time and males have lower ESR values than females. REFERENCES
The following images related to this document are available:Photo images[ja10004t3.jpg] [ja10004t4.jpg] [ja10004t1.jpg] [ja10004t2.jpg] [ja10004t5.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}