 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Health Sciences, Vol. 12, No. 1-2, Jan-June, 2005, pp. 1-12 Health economics: potential applications in HIV/AIDS control in Africa Joses M. Kirigia1*, Luis G. Sambo2, Emilienne Anikpo 3, Eddie Karisa4 and Germano Mwabu5 1Health Economist, World Health Organization, Regional Office for Africa (WHO/AFRO); 2 Regional Director, WHO/AFRO; 3 Senior Advisor, Health Action in Crisis Development, WHO/HQ; 4 Former Long-term Health Development Economist, Health in Sustainable Development Unit, DES; 5Professor
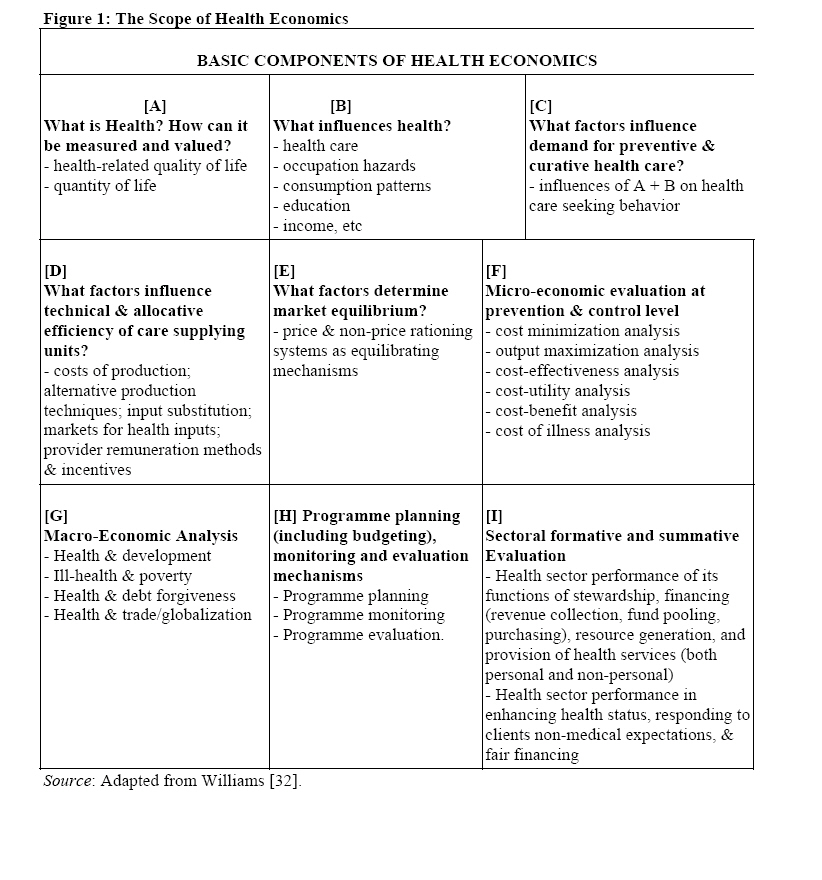
of Economics, Department of Economics, University of Nairobi. Code Number: jh05002 SUMMARY There is growing evidence that HIV/AIDS has enormous negative impact on health status and economic development of individuals, households, communities and nations in the African region [33]. Thus, there is urgent need for various disciplines to demonstrate how they can contribute in curbing the spread of this deadly disease in the African region. This paper, using an extended version of Professor Alan Williams [32] schema as the conceptual framework, attempts to demonstrate how health economics can be used to inform policy and managerial choices related to HIV/AIDS advocacy, prevention, treatment and management. It argues that the discipline of health economics (and economics generally) is extremely valuable in: measuring health impacts of the disease and interventions; evaluating the relationships between health care-seeking behaviour of individuals and health system specific attributes; the estimation of determinants of compliance of HIV/AIDS patients with treatment regimen; establishing of health institutions efficiency in combating AIDS; guiding choices of HIV/AIDS interventions; assessing the relationships between HIV/AIDS, development, poverty, and trade; programme planning, monitoring and evaluation; and assessing health system’s overall performance. The paper is a modest attempt to show how the discipline of health economics can elucidate, and help in resolving practical and conceptual issues in HIV/AIDS control in Africa. Introduction Neither individuals nor governments have enough resources to tackle the HIV/AIDS pandemic. It is therefore impossible to avoid making choices concerning how best to use the available resources. Health economics is concerned with choice in the context of health maintenance when resources are scarce. The objective of this paper is to demonstrate how health economics can be used to inform policy and managerial choices related to HIV/AIDS advocacy, prevention and management. The discussion in text is in relation to Appendix Figure 1. Health and health Indices (Figure 1: Box A and B) Over the last decade and half health economists have attempted to answer the questions posed in Figure 1. This subsection addresses (albeit superficially) the questions posed in Box A and B, which include: What is Health? How can it be measured and valued? What influences health? The World Health Organization [1] defines health as a “state of complete physical, mental and social well-being, and not merely the absence of disease or infirmity”. Social scientists define health as the ability to perform one’s societal expected roles or functions [2-4]. HIV/AIDS opportunistic infections inhibit patients mobility, capacity for social participation (partly due to stigma), performance of usual activities (e.g. work or schooling), ability for self-care (especially during the severe stage) and causes them pain/discomfort (psychological and physical) plus anxiety/depression (own and close family members). In short, HIV/AIDS predisposes individuals to sub-optimal quality of life (QoL) and length of life (LoL). Thus, in the context of HIV/AIDS, an ideal health index is the one that combines changes in both QoL and LoL due to HIV/AIDS onset or intervention. Examples of such indices are quality adjusted life years (QALY) [5-7]; disability adjusted life years (DALY) [8]; or disability adjusted life expectancy (DALE) [9]. In 1998, for instance, HIV/AIDS caused 1.83 million deaths translating into 54.101 million DALYs lost in the WHO African Region alone. The effect of HIV/AIDS or intervention will be the difference between total expected DALE without HIV/AIDS (with intervention) and total expected DALE with the disease/condition (or without intervention). An individual’s health is a function of many factors, the most important being the following:
Unfortunately, there is dearth of evidence on the extent to which social (including cultural, health and education), environmental, political, and economic systems and institutions in the African Region promote HIV/AIDS victims respect, dignity, integrity, and self-determination. This is a grey area that requires research. Individual and household Demand for health care (Box C) Scarcity necessitates choices of many different forms. At a general level, as individuals or households, we must decide how to use the resources that we have: our physical (e.g. land, equipment) and intellectual (e.g. knowledge and skills) assets, our material wealth, and our labour time. Box C in Figure 1 delves into the analyses of individuals and households health-related demand/choices. In the context of HIV/AIDS, an individual faces various choices: As a non-infected woman, given the high HIV/AIDS prevalence within my community, should I ask a new partner or an old one to use condoms during a sexual encounter so as to reduce the probability of infection? As a male, should I use condoms during extra-marital sexual encounters or not? As a HIV/AIDS positive person, should I disclose my status to my partner and/or community or not? Given my positive HIV/AIDS status, should I use a condom in a sexual encounter to avoid infecting a partner? As a HIV/AIDS positive person, should I seek treatment from modern health facilities or a herbalist or a spiritual healer? If I opt to seek Western health care, should I visit a tertiary hospital, a regional hospital, a district hospital, a health centre, a dispensary, or a nursing home? Which anti-retro-viral drug should I use? Should I comply fully with the prescribed anti retroviral drugs or not? If I opt to consult a traditional healer, which one should I visit? Given that I am HIV/AIDS positive and addicted to intravenous illicit drugs, should I spread the virus to other drug addicts by sharing injection needles and syringes or not? As a HIV/AIDS positive household head, how much of the household resources should be spent on prolonging my life? Unfortunately, there has been limited appreciation among economists and laymen alike, of the potential usefulness of the above theoretical choice questions in the prevention and control of HIV/AIDS. Choice analysis is based on the assumption that people behave rationally, that is, individuals are rational decision makers. Rationality means that people are capable of setting goals and of acting in a manner consistent with the achievement of those goals [10]. Concerning the HIV/AIDS-related choices mentioned above, economics tells us that individuals will choose the alternative for which they believe the net gain (utility) to be the greatest. In other words, all consumers (irrespective of their social status) have a common objective – to do what is best for themselves or their families with the resources under their control. Choice of a particular commodity or course of action (e.g. whether or not to use a condom) is usually assumed, in health economics (and in economics generally), to be a function of personal socio-economic characteristics (e.g. age, marital status, religion, health education, secular education, income, risk attitudes, epidemiological environment, genetic endowment, etc), and commodity-level attributes (e.g. service price, travel cost to service source, waiting time at the source, perceived effectiveness of service, etc). Economists employ a number of methods, typically of a statistical nature) to establish the causal-effect relationship between choices made by individuals (dependent variables) and the variables that help explain those choices. Kirigia and Sayed [11] estimation of qualitative response models (using a random sample of general South African adult population) revealed that respondent’s race, gender, marital status, smoking status, beer drinking status, income, price at the facility normally visited, travel time to the source of condoms, and self-assessed health status were highly significant predictors of demand for condoms. This study highlighted the need for developmental programs aimed at raising incomes and improving access to modern health care services for the S. Africans who were discriminated against during the apartheid era. Kirigia and Muthuri [12] fitted linear probability and logistic models on random samples of South African married and single women to estimate the impact of social, economic and educational factors on the likelihood of woman’s decision to ask a new partner to use condoms during sexual intercourse in order to reduce the probability of HIV infection. The study revealed that the knowledge that: condoms have a contraceptive benefit; AIDS epidemic is spreading rapidly across S. Africa; people in ones own community are using condoms to avoid getting AIDS; and AIDS can be transmitted by having sexual intercourse without using a condom had positive and statistically significant effect on the decision to use a condom. The authors concluded that equipping women with those forms of knowledge would go a long way in empowering them to exercise their rights to safer sexual relationships. Demand analysis is widely used to explain use of addictive substances [13,14], contraceptives [15], toilets [16] and human organs. Informed use of these methods can greatly enhance targeting of health-related interventions geared at modifying human behaviour, including sexual habits that expose individuals to a high risk of HIV infection. Supply of Health Care (Box D) Supply refers to the maximum quantity of health services firms/health units are able to produce and are willing to sell at the going market prices. The quantity willingly supplied during a specified period of time is positively related to market prices, ceteris paribus. A higher price gives profit-motivated producers (e.g. private health care providers) the incentive to increase production. In addition, in the short run, the quantity supplied is affected by input prices, technology and prices of other goods. Underlying the supply of any good or service is the production function, that is, the relation between the output of that good or service and the resources (or inputs) used to produce it. If the output were outpatient and inpatient care, then included in the inputs would be the number of and type of physicians, nurses, technicians, pharmaceutical supplies, non-pharmaceutical supplies, beds, space, etc. To some extent the various types of technical personnel are substitutable for one another, although not on one-to-one basis. Since the resources are scarce, allocating more resources to HIV/AIDS control means allocating less to the prevention and treatment of other diseases, for example, other communicable and non-communicable diseases. The opportunity cost of reducing AIDS-related DALYs lost is the number of DALYs that would have been averted if the same resources were invested in, for example, immunization of children. Whereas more HIV/AIDS-related DALYs would be averted through the available preventive cost-effective interventions, the same cannot be said for HIV/AIDS treatment, in the absence of effective cure. Even for public health care providers, who are not profit-but service-driven, given that health producing inputs are available in limited supplies, it is critically necessary to use them efficiently to produce outputs (whether defined in terms of mortality and morbidity reduction, prevalence or incidence reduction, or in terms of health indices). Inefficiencies of any form represent wasted opportunities for improving at least one citizen’s health status at no extra cost, which in itself can also be considered unethical and immoral. For example, inefficiencies in use of health facility resources represent lost opportunities for investing wasted resources in the prevention of HIV/AIDS and other diseases. The sub-discipline of health economics often uses mathematical (linear, integer and goal) programming methods to estimate efficiency scores and excess inputs (or output deficit) for individual decision making units, e.g. hospitals, health centres, dispensaries, clinics, programs, etc. Kirigia, Lambo and Sambo [17]; Kirigia, Sambo and Scheel [18]; and Kirigia, Sambo and Emrouznejad [19] are examples of African studies that have used Data Envelopment Analysis (DEA) in estimating magnitudes of inefficiencies among individual hospitals and clinics in South Africa and Kenya. If the health care policy-makers have the will, they can easily re-allocate excess technical human resources to those provinces and districts with heavy caseloads of HIV/AIDS. Micro-economic evaluation at prevention &control level (Box F) Economic evaluation is a comparative analysis of costs and consequences of at least two or more interventions into HIV/AIDS, for example. There are five main economic evaluation methods:
Although total cost of illness (TCOI) studies do not qualify as economic evaluations, they will be discussed in this paper with a view to inform, and hopefully correct misconceptions regarding their scope in health policy analysis. Total cost of Illness (TCOI) The essence of TCOI studies is recognition, identification, listing, measurement and valuation of costs generated by an illness, e.g. AIDS. Such studies heighten awareness of a health problem and the need for its insertion in a list of priorities. In the context of HIV/AIDS, such studies can help focus society’s attention on economic impact of the pandemic. It is appropriate to estimate TCOI when the question facing health care policy-makers is: how much money does HIV/AIDS cost a given society (if societal viewpoint is assumed) per year? The TCOI studies involve mainly two stages: (i) identification of all cases of the illness in question, e.g. HIV/AIDS. The potential sources of data are: national statistics (e.g. from National Health Information Systems) or extrapolation to the whole population from a small survey. The challenges in obtaining such epidemiological data are: difficulty in case definition; incomplete knowledge of the natural history of the disease; and under-notification of HIV/AIDS cases. (ii) Identification of costs generated by all cases of HIV/AIDS, including: direct costs (borne by the health care system, community and family in directly addressing the problem); indirect costs: mainly productivity losses caused by the problem or diseases, borne by the individual, family, society and by the employer; and intangible costs - usually costs of pain, grief, suffering and loss of leisure time. In collecting cost information, analysts can use either the incidence approach, i.e. estimate costs of cases from their onset to disappearance (due to cure or death); or prevalence approach, i.e. estimate costs of all cases in a short period irrespective of the stage they are at. TCOI methodology has been castigated for various reasons [20]:
Cost Minimization Analysis (CMA) CMA is the art of identifying the least costly intervention option (or policy) when there is evidence that options under consideration are equally effective in achieving the desired objective. It is appropriate when the policy question to be answered is: "Given that we must achieve a specific level of output, what is the least costly way of realizing it, given two (or more) equally effective options?" The data requirements include: epidemiological evidence, preferably from randomized controlled trials (RCT), that the effectiveness of competing options is equal; direct costs, indirect costs (time lost from work) and intangible costs (anxiety, pain). If HIV/AIDS programme manager is faced with ‘n’ preventive or treatment options, CMA decision criteria requires that, if IC2 < IC1 <.. An analyst who decides to apply CMA to HIV/AIDS (or any other disease) may not have evidence that the 'ultimate' effectiveness of competing options is equal. Output Maximization Analysis (OMA) OMA is the art of identifying the health care option with the highest amount of expected output from a given level of resource endowment. It would be appropriate if the problem facing a HIV/AIDS decision-maker was: "Given that the options under evaluation have equal cost, which option promises the highest level of output?" The data requirements are: evidence that competing options have equal cost; and effectiveness (measured in an appropriate index) without and with alternative policies. Since the options under consideration have equal cost, the decision criteria becomes: if E1 > E2 > En, choose option 1; where Ei is the effectiveness of ith intervention. The potential analytical problems are: evidence that direct costs, indirect costs (time lost from work), intangible costs (anxiety, pain) are equal may be lacking; and unless effectiveness is expressed into a common yardstick, OMA cannot be used in choosing between options with disparate outcomes. For example, this form of economic evaluation cannot inform the choice between preventive and treatment HIV/AIDS intervention options. Cost-Effective Analysis (CEA) CEA compares two or more interventions, measuring the inputs in monetary terms and the outcomes in natural or physical units. CEA is appropriate when one of the following conditions holds: there is one, unambiguous objective of the intervention(s), and therefore a clear dimension along which effectiveness can be assessed; there are many objectives, but that the alternative interventions are thought to achieve these to the same extent; or the problem facing a decision-maker is: Given that we are not sure what level of performance to aim at, or what level of resources will be at our disposal, and we have no way of valuing the benefits, which option should be given priority?" CEA data requirements are: direct costs, indirect costs (time lost from work), intangible costs (anxiety, pain), and externality costs; and outcomes measured in natural units such as lives saved / deaths averted, years of life saved, cases detected and treated, cases prevented, visits, discharges, cures, etc. The CEA decision criteria requires an analyst to recommend choice of option 1 if δC/δE1 < δC/δE2 < ....< δC/δEn; where δCi is the incremental cost of intervention i (i=1,..,n) and δEi is the incremental effectiveness of ith intervention. Thus, the policy with least incremental cost-effectiveness ratio is preferred. CEA methodological issues are: it does not resolve the problem of option selection whenever different options yield more than one kind of beneficial effect with the mix of benefits differing between options; it gives no guide as to whether interventions should be implemented at all even though it is possible to rank options to meet a specific objective; and its inability to compare the benefits of an option with the opportunity cost. Cost Utility Analysis (CUA) CUA is a method that compares two or more interventions, measuring inputs in monetary terms and the outcomes in an health index, e.g. quality adjusted life years (QALYs), disability adjusted life years (DALYs) or disability adjusted life expectancy (DALE). This method is appropriate when:
CUA, like other full economic evaluation methods, depending on the perspective of the analysis would entail collection of direct, indirect (time lost from work), intangible (anxiety, pain), and externality costs. It would entail listing inputs (consumed or required), quantifying and valuing them at the going market prices. If the study is retrospective, one would need to obtain actual quantities and values of inputs consumed by each intervention being appraised. Data for this kind of study can be obtained from financial records in program manager’s office and activity data from the records, e.g. of number of people treated, etc. On the other hand, if it is a prospective/futuristic study, the analyst will need to estimate the quantities and values of input requirements for each intervention under evaluation. For prospective studies, quantities (by type) of inputs (by intervention) can be generated through interactive interviews with experts (e.g. program managers, epidemiologists, public health officers, etc.). On the effectiveness side of the equation, data requirements will depend on the health index that one decides to use. If one decides to measure outcomes measured in QALYs, one would need: descriptions of various HIV/AIDS-related health states covering various quality of life dimensions; health state utilities; probability of experiencing each state with and without intervention; population at risk of infection; and discount factors for each year under consideration [2,5]. Health status utilities can be obtained through household surveys [3]. Probabilities of experiencing each state with and without intervention can be obtained from either clinical trials and randomized controlled trials; literature through meta-analysis; or experts through a Delphi approach [5]. The CUA decision criteria dictates that all the interventions under consideration be ranked on the basis of their incremental cost-utility ratios (ICUR), i.e. ICUR = (CAI -CSQ)/(QALYAI -QALYSQ) = δC/δQALY where CAI is cost of alternative intervention i; CSQ is the cost of the status quo, i.e., no intervention; QALYAI is quality adjusted life years expected from alternative intervention i; QALYSQ is those from SQ; and δ means ‘change in’. The HIV/AIDS intervention with the least ICUR should be should chosen, all other considerations held constant. There are a number of issues surrounding CUA methodology and it application, namely: field of cost-utility analysis is relatively young and the methodology is still developing; it can only be used in pursuit of production and product-mix efficiency, but not efficiency in exchange, mainly because cost and benefits are not measured in a common yardstick; construction of culturally acceptable qualify of life measurement instrument; and administration of a quality of life instrument where majority of the people are illiterate. In spite of the above methodological hurdles, CUA technique has effectively been used in Kenya to identify the optimal schistosomiasis intervention strategy [21], and thus, there is no reason as to why it cannot be applied to HIV/AIDS in Africa. Cost-Benefit Analysis (CBA) CBA is the technique employed in identifying, quantifying, and valuing in a common yard-stick (usually local currency) all important costs (direct, indirect, intangible and externality costs) and consequences (benefits) to society of any potential or actual change in resource allocation in the economy. It is appropriate to use when the problem facing a decision maker is whether a single intervention policy or a number of intervention policies are worth implementing i.e when an issue is whether benefits are greater or equal to costs. Examples of CBA policy questions are:
Within CBA methodology intervention benefits are measured in money (especially in local currencies) using either the ‘human capital’ approach [22], the ‘implied values’ approach, or the ‘willingness to pay’ approach [23,24]. In recommending HIV/AIDS interventions for implementation, the analyst can use either of the following three decision criteria: (i) net present value (NPV), whose decision rule is to accept the option being evaluated if NPV > 0; (ii) benefit-cost ratio (B/C), whose decision rule is to accept the option being evaluated if B/C > 1; or internal rate of return (IRR), i.e., the rate of interest “R” for which NPV=0, whose decision rule is to accept an intervention if R > r. CBA can be used: to address all efficiency issues - efficiency in production, product-mix, and exchange; to aid HIV/AIDS programme managers decide whether a single intervention or multiple interventions are worth implementing; and to identify the option with the greatest expected net benefits. CBA has a number of methodological issues surrounding it: measurement and valuation of interventions benefits; valuation of statistical life; derivation of a social welfare function from individual utility functions; incorporation of equity concerns; uncertainty and time preference; and CBA decision rules. Economic evaluations:
Furthermore, economic evaluation can provide information for making informed decisions with regard to the following:
Macro-economic Analysis (Box G) HIV-AIDS and development Professor Michael Todaro [25] identifies the three dimensions of development as: economic growth (EG); growth in people’s self-esteem through the establishment of responsive health, social, cultural, political, and economic systems and institutions that promote human dignity and respect; and increase in people’s freedom by empowering them to be masters of their own destiny, i.e. in terms of making choices related to livelihood, health care, political and civil leadership, religion, self-expression, friends/associates, etc. HIV/AIDS has a number of negative effects on development. Firstly, it depletes quality and quantity of human resources, and thus, economic productivity. Secondly, it relegates its victims to a culture of social and economic dependence leading to a reduction in their self-esteem or self-worth. Lastly, the condition deprives its victims of the freedom from avoidable ill-health and from escapable mortality. The discipline of economics would be useful in estimating the causal-effect relationship between the number of HIV/AIDS cases and economic growth; HIV/AIDs and levels of self-esteem among individuals and communities; HIV/AIDS and the degree of freedom in making various choices; and the degree of responsiveness of public institutions to HIV/AIDS patients rational expectations. Kirigia, Sambo, Okorosobo and Mwabu [26] is an example of a study that used regression analysis to estimate the impact of HIV/AIDS morbidity and mortality on individual African countries gross domestic product (GDP). HIV-AIDS and poverty Poverty predisposes the poor to HIV infection through inaccessibility to preventive information and commodities; “forced” migration (in search of paid jobs), and need to embark on high-risk economic behaviour (e.g., commercial sex) and social behaviour that increase the risk of infection (e.g., alcohol consumption and drug use). Once infected, AIDS exposes its victims to income poverty via productivity losses (resulting from reduced stamina, absenteeism and death), diminished productivity due to national income reductions; increased dependency ratio, as the productive portion of the population decreases; increased number of orphans, and hence, the cost of taking care of them; catastrophic health care costs, and hence, diversion of resources from economic growth-generating activities; overload of national health systems, and hence, their capacity to respond effectively to increased needs. Using econometric methods, health economists can study the magnitudes of causal-effect relationship between HIV-AIDS and various forms of human deprivations. Such studies would inform the policy-makers on how various HIV-AIDS interventions impact on poverty levels. HIV-AIDS and Debt Forgiveness HIV-AIDS is not selective when depleting human capital or resources, and thus, it is a problem of all social (e.g., health, education, etc.) and productive (e.g., commerce, industry, agriculture, tourism, etc.) sectors. And this is why the problem requires a multi-sectoral approach to address it. Since majority of the countries in the Region are Highly Indebted Poor Countries (HIPC), they are eligible for varying degrees of debt-relief, and therefore, there is a need for ensuring that all sectors invest some of the HIPC funds (hoping they are not just ‘virtual’ funds) into HIV-AIDS prevention and management. Health economics would be useful in identifying the most cost-effective interventions or the so-called ‘best-buys’. HIV-AIDS and Trade Trade is about exchange of commodities (goods and services) between individuals, communities, or countries. International trade is about exchange of commodities between sovereign states. Most of the countries in the African Region export raw or semi-processed materials to the developed countries and the proceeds are used to import a variety of manufactured commodities, including motor vehicles, medical equipment, drugs, etc. Unfortunately, the process of producing those exports is highly labour-intensive, meaning that depletion of the quantity and quality of labour through AIDS-related infections would also reduce the quantity of exports. This in turn, leads to a reduction in the amounts of foreign currency required for importing pharmaceutical and non-pharmaceutical supplies needed in the prevention and management of diseases, such as, HIV-AIDS. On the other hand, since HIV-AIDS has no respect for geographical boundaries, the movement of traders between countries acts as a vehicle for transmitting HIV-AIDS. Once again, quantitative economics methods become useful in quantifying the causal-effect relationship between changes in numbers of HIV-AIDS cases, and volumes (or value) of exports and imports. Program planning, budgeting, monitoring and evaluation mechanisms (Box H) A plan is a course of action consisting of objective(s), target(s), expected result(s), activities, resources and a monitoring/evaluation element. An objective is an end result that a program seeks to achieve, whereas a target is a quantified specific objective to be reached within a given time frame. A result is an observable and measurable outcome produced by an activity or a set of activities, an activity being a set of related tasks aimed at producing a result [27]. A budget is a detailed list of quantities and monetary values of different types of inputs required to implement each planned activity. The objectives of an HIV/AIDS monitoring process are
Evaluation is the assessment of effectiveness, relevance, quality, adequacy, utilization and efficiency of an HIV/AIDS programme [28]. HIV/AIDS prevention and management does not occur in a vacuum; instead, it occurs within the health system. The effectiveness of a HIV/AIDS programme (and all other health programmes) largely hinges on the effectiveness of the underlying health system. This is why it is necessary to assess the extent of health system performance in enhancing health status of populations; responding to clients (including those who are HIV positive) non-medical expectations; and fairness in financing [29]. Health system performance assessment entails knowledge of economics, among other disciplines. Knowledge of health economics is also necessary (but probably not sufficient) in the analysis of the functions of health systems, including: stewardship [30], resource generation, financing (revenue collection, fund pooling and purchasing) [31] and provision of personal and non-personal health services [29]. Conclusion In the context of HIV/AIDS, the discipline of economics is critically important in the process of measuring health impacts of the disease and interventions; evaluating the causal-effect relationship between health care-seeking behaviour and individuals and health system specific attributes; the estimation of the statistical association between patient compliance with intervention (e.g., treatment regimen) and personal as well as intervention-specific attributes; establishing individual health institution’s magnitude of inefficiency in resource use; guiding choice of HIV/AIDS interventions, i.e. identifying the best buys; assessing the macro-economic relationship between HIV/AIDS, development, poverty, and trade; programme planning, budgeting, monitoring and evaluation; and the assessment of health systems performance. Acknowledgments This paper has benefited greatly from the lectures and other works of Professors Tony Culyer, Mike Drummond, John Posnett, Alan Maynard, Alan Williams and Andrew Jones of the University of York (UK) and Gavin Mooney (CTT) of Curtain University (Australia). This paper is dedicated to health care personnel and community-based care givers in the Africa Region who courageously care for victims of AIDS, while simultaneously teaching the people how to avoid HIV infections. We owe profound gratitude to Jehovah Maccadeshem for inspiring and enabling us to write this paper. The opinions expressed in this article are those of the authors and should not be attributed to either WHO or any of the acknowledged. References
Copyright 2005 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh05002f1.jpg] |
| |||||||||

{kind=link}