 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
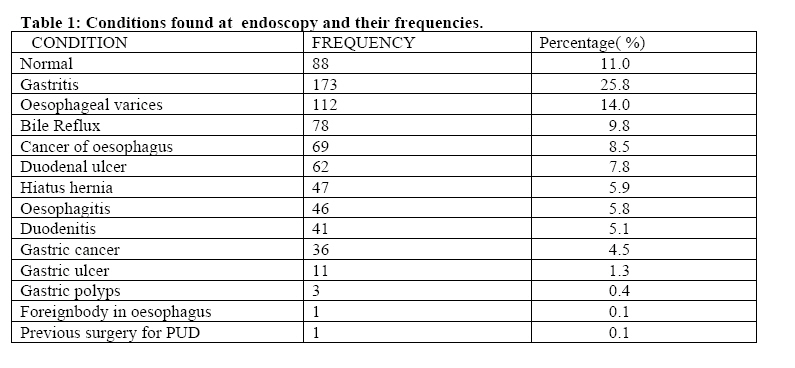
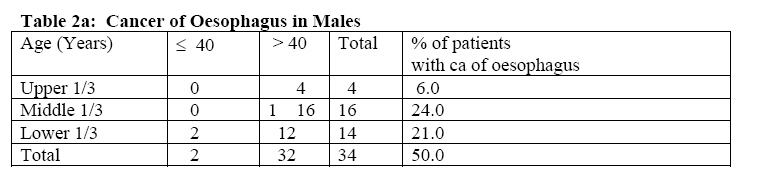
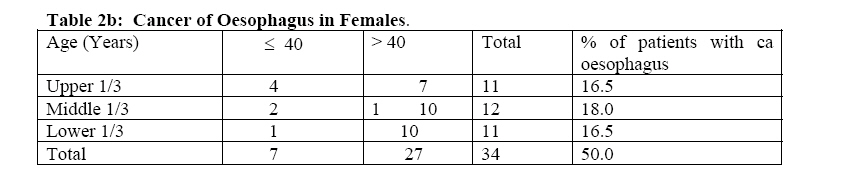
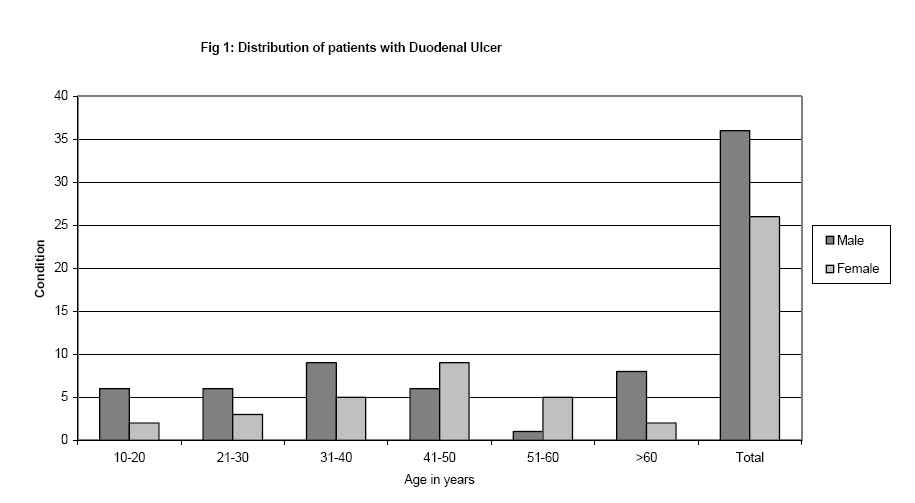
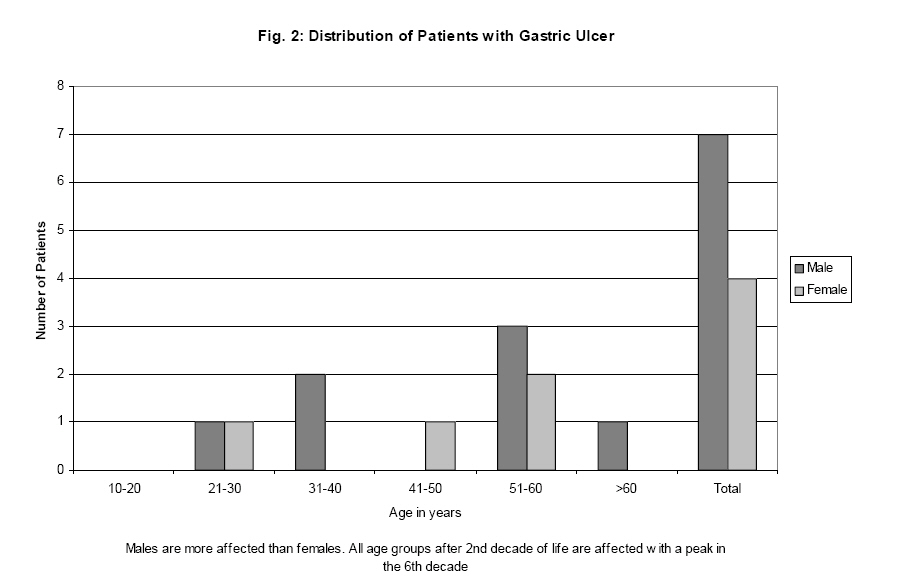
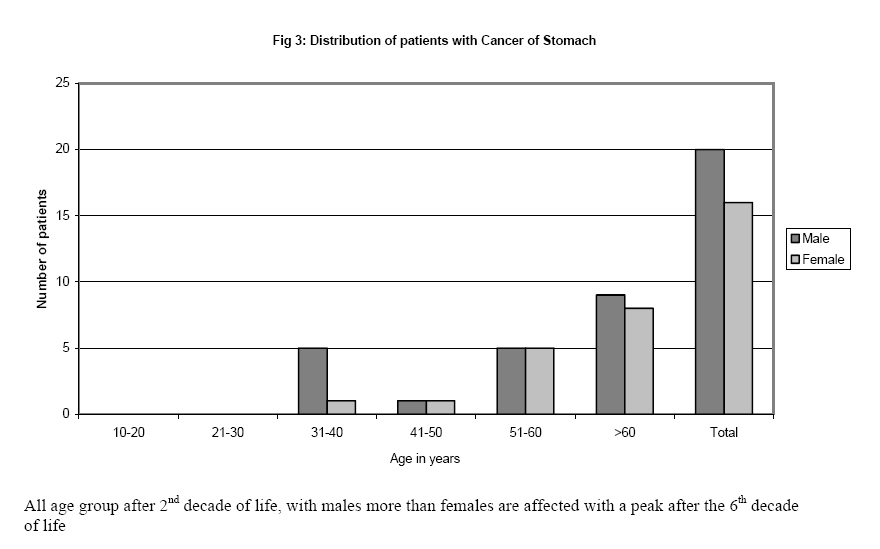
African Journal of Health Sciences, Vol. 12, No. 1-2, Jan-June, 2005, pp. 49-54 Patterns of upper gastrointestinal diseases based on endoscopy in the period 1998-2001 Hudson Lodenyo1 , Fasana Rana2, Geoffrey Z. Mutuma1, John M Kabanga1, Julius K Kuria1, and Fredrick A. Okoth1. 1. Kenya Medical Research Institute, P.O. Box 54840, Nairobi; 2; University of Nairobi, P.O.Box 30197, Nairobi Code Number: jh05008 SUMMARY Upper gastrointestinal complaints are common in Kenya. Though these have remained unchanged over the last 20 years, the pattern of upper gastrointestinal disease on endoscopic examination seems to be changing. There appears to be progressive increase in oesophagitis and cancer of the stomach. Peptic ulcer disease has remained stable while Cancer of the oesophagus is still common. The paper intends to report on endoscopic findings at the Centre for Clinical Research, Kenya Medical Research Institute (KEMRI) over the period October 1998 and May 2001. The sources of information are records made at the time of endoscopy and histology reports on biopsies taken. Seven hundred and sixty eight patients were endoscoped. The male to female ratio was 1.7:1 with mean age ±SD of 40.8 ±20.1 years and age range was 3 to 96 years. Majority of the patients had abnormal findings with gastritis being the most common ( 25.8%). It is concluded that gastritis is an important cause of morbidity in Kenya. Oesophagitis, mainly due to gastroesopahageal reflux disease, seems to be on the increase. Gastric cancer is not as rare as previously thought and peptic ulcer disease is still common. Introduction Upper Gastrointestinal complaints are common in Kenya. These include dyspepsia, dyspehagia, flatulence, heartburn, haematemesis and odynophagia. Though complaints have remained unchanged, the pattern of upper gastrointestinal disease in Africa on endoscopic examination seems to be changing. There seems to be a progressive increase in both infective and acid related oesophagitis while peptic ulcer has remained relatively stable [1-3]. In his report from Ethiopia in 1981 Tsega found oesophagitis in less than 1% of those endoscoped [1]. In 1991, reports by Ogutu and colleagues from Kenyatta National Hospital indicate that oesophagitis was found in 4.2% of those presenting with dyspepsia [3]. Kodjoh and colleagues in 1991 in Cotonou, Benin reported oesophagitis in 21.5% of the 930 patients who underwent endoscopic examination [4] while Missalek found it in 27% of his patients [5] and Olubuyide reported 14% [6]. Frequency of peptic ulcer disease was variable as found by Tsega in Ethiopia and Ogutu in KNH, Nairobi [1,3]. There is therefore need to audit our reports on endoscopic examination regularly. Methodology This is a report on analysis of upper gastrointestinal endoscopic findings between October 1998 and May 2001 in our endoscopy unit. The patients were referred from hospitals around the country, private clinics and Kenyatta National Hospital. Patients gave informed consent for the conduct of the examination. Overnight fasting was an essential requirement. Diagnostic procedures were done after oral pharyngeal anaesthesia using xylocaine spray (ASTRA). Those who required variceal injection sclerotherapy were given pethidine, midazolum and hyoscine butylbromide all intravenously in addition to the xylocaine spray. Findings at endoscopy were recorded in a procedure record book by the doctor who performed the procedure in a structured manner where name; age, sex, indication for procedure, procedure performed, findings and recommendations are recorded. All biopsy specimens were processed in the KEMRI histology laboratory and examined by a pathologist for histological diagnosis. Results Males were more than females with male to female ratio of 1.7:1 and mean age ±SD was 40.8 ±20.1 and range of 3-96 years. Gastritis was the most frequent finding accounting for 25.8 % and foreign body in oesophagus was the least accounting for 0.1% as shown in table 1. Esophageal varices accounted for significant upper gastrointestinal morbidity (14%). Peptic ulcer disease & duodenitis combined account for 14.1% of our findings underlining their importance as causes of morbidity in our patients. Gastric cancer, rare 20 years ago, accounted for 4.5%. Cancer of oesophagus is still common (see table 1) Tables 2a and b show that fairly young people are also affected by cancer of oesophagus in our set up with as many as 13% aged below 40 yrs. The middle third is still the most frequently involved part of oesophagus followed by the lower third. The frequency of neoplasm in the upper third seems to be more in females than in males (M: F of 1:2.8). The involvement of the upper third of the oesophagus also tend to affect younger females than males. Duodenal ulcer is still common in our patients. All age groups are affected with males predominating (fig 1 ). Again, all age groups after 2nd decade of life are affected by gastric ulcer with a peak in the 6th decade. Males are more affected than females (fig 2 ). Cancer of the stomach affects all age groups after second decade of life. Males are more affected than females (fig 3 ). Discussion Oesophagitis, a condition that was uncommon in Eastern Africa 20 years ago is increasingly becoming common. Tsega in 1981 in Addis Ababa found oesophagitis in less than 1% of patients [1] Ogutu and colleagues found it in 4.2% of those examined in 1997 [3] and we found it in 5.6% of those endoscoped. Cancer of the stomach was also less common 20 years ago (<1% (1981) Vs 4.5 % in this study) than now. Oesophageal varices, mainly due to portal hypertension secondary to schistosomal liver disease, still remain a significant cause of morbidity [1-3]. Bile reflux gastritis is a significant cause of dyspepsia found in as many as 9.6% of those endoscoped. Duodenal ulcer is still common in our set up. Benign gastric ulcer still remains rare as it was 20 years ago [1]. Hiatus hernia seems to be gradually increasing. Inflamed gastric mucosa, mainly due to helicobacter pylori, has remained common, found in up to 25% of those examined. Gastritis is mainly H.pylori related as shown by Ogutu [3]. Cancer of the oesophagus, mainly squamous cell type, is still common in Eastern Africa as shown by Tsega, [1] and in our findings. Gastric polyps and achalasia cardia remain uncommon. Conclusion Gastritis is an important cause of morbidity in Kenya. Oesophagitis mainly due to gastroeosophageal reflux disease seems to be on the increase. Gastric cancer is not as rare as previously thought. Recommendations
Acknowledgement We wish to acknowledge the following:, Our patients; Josephine Kesusu for computer services; Nursing staff at the Center for Clinical Research (CCR) and Director KEMRI. References
Copyright 2005 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh05008f1.jpg] [jh05008t2a.jpg] [jh05008t1.jpg] [jh05008t2b.jpg] [jh05008f3.jpg] [jh05008f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}