 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Health Sciences, Vol. 13, No. 1-2, Jan-June, 2006, pp. 96-100 A skin colour code for the Nigerian (Negroid) population Adekunle O George* and Adebola O Ogunbiyi Department of Medicine, Dermatology Unit, University College Hospital, Ibadan,
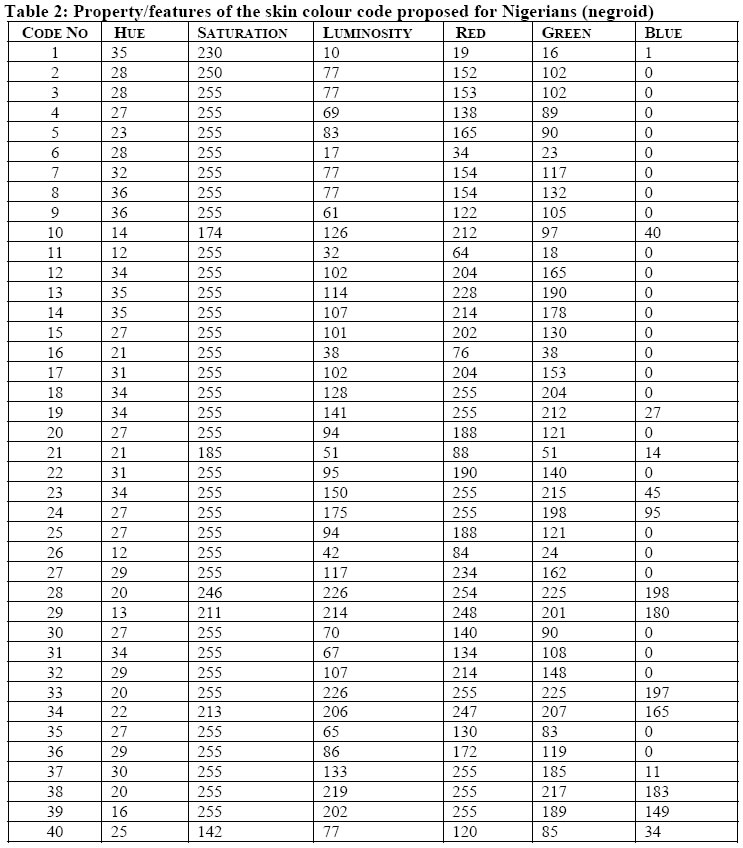
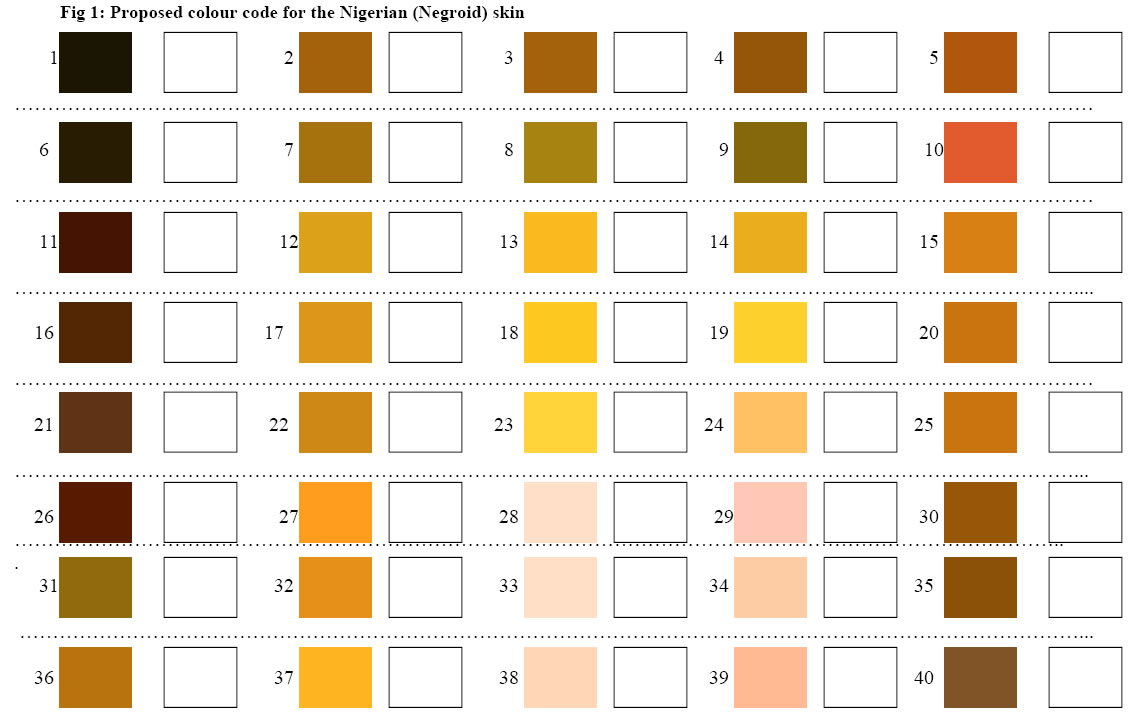
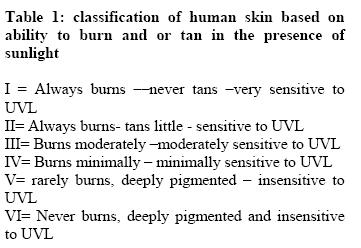
Nigeria. Code Number: jh06013 SUMMARY Some researchers have codified various people of different racial and pigment backgrounds into skin types. The West African native population generally falls into type VI –least likely to burn. There is a need for skin colour code in a multiethnic country like Nigeria especially for the purpose of health matters. The human eye is still the most accurate instrument for the measurement of colour; its interpretation however is subjective. An objective form of documentation is needed that will be simple, quick and inexpensive. To meet the challenge for the development of a skin colour code for Nigerians, a study was conducted at the University College Hospital (UCH) Ibadan, Nigeria. The study aimed at visually identifying possible skin colours and to reproduce this on the computer. 40 colour chips were identified and found relevant for the Negroid skin in Nigeria including the Nigerian albino. The chart can be laminated using thin transparent plastic film to prevent transmission of infection from skin to skin in different people. A skin colour code can be useful for clinical evaluation of disease conditions like vitiligo as well as for epidemiological studies. Its diagnostic potential is yet to be assessed.[Afr J Health Sci, 2006; 13:96-100] Introduction The principal pigment determining skin colour is melanin. The chemistry, aggregation, and distribution of melanin are the major factors that determine colour and hue of cutaneous pigmentation. Three other pigments that contribute to normal skin colour are oxygenated haemoglobin, reduced haemoglobin and carotenoids. Some researchers [1] have codified various people of different racial and pigment backgrounds into skin types as seen in Table 1. The West African native population generally falls into type VI – least likely to burn. There is a need for skin colour code in a multiethnic country like Nigeria especially for the purpose of health matters. Pearson working in Igboora, a rural area in south-western Nigeria [2] observed hypochromia- (hypopigmentation) - especially on the face as an accompaniment of tuberculosis. He further wrote “Though the human eye is still the most accurate instrument for the measurement of colour [3] its interpretation is subjective”. The unaided human eye under the best possible viewing conditions, comparing large areas of colour in good illumination using both eyes can distinguish 10, 000 different colour surfaces [4]. The most accurate photo electric spectro- photo meters possess a precision of only 40 % of the human eyes [4]. If hypochromia is to be useful in general outpatient and tuberculosis clinics for differential diagnosis and assessment of progress of patients, Pearson suggested that “an objective form of documentation must be found that will be simple, quick and inexpensive’’[(2]. To meet the challenge for the development of a skin colour code for the Nigerians, a study was conducted at the University College Hospital (UCH) Ibadan, Nigeria. The aim of this phase of the study is not to relate diseases to colour changes as Pearson tried to but to assess the spectrum of skin colour in healthy normal Nigerians Method/subjects The study aimed at visually identifying possible skin colours in apparently healthy Nigerians and to reproduce these colours on a personal computer using the data obtained. The study was conducted at the University College Hospital (UCH), Ibadan, Nigeria, within the period January 2002 to May 2002. Nigerians belong to the Negroid race. It is possible to vary the factors related to colours – hue, intensity, saturation etc in over 500 combinations. The authors looked at skin colours of various subjects in the environment. Since skin colour varies slightly from one anatomical area of the body to another, the face (the cheek) was used to standardized the data obtainable. Individuals whose facial complexion from the practical point had not been affected /altered by ‘makeup’ –powder puff, rouge and the like were selected for assessment of their skin colour. The colours observed were matched with numerous possibilities produced earlier on a computer /colour printer set. Identical rectangular boxes adjacent to the coloured- filled boxes were cut to enable the viewing of the skin of the face and the matching of colours.. The Munsell colour scheme for skin, hairs and eyes used by Pearson in his study had circular 9-mm holes in the card besides each colour chip. While he used an X-ray viewing box for the purpose of standardization, natural light was adopted in this study since a viewing box may not be available in many primary health centers in Nigeria and electricity may be lacking. Pearson adopted an industrial type colorimeter. He used one with a flexible glass fiber light lead (Lovibond Flexible optic Tintometer), which facilitated clinical application. Results 40 colour chips were identified over the study period and found relevant for the spectrum of the Negroid skin colour in Nigeria including the Nigerian albino (table 2 and fig. 1). However the majority (91.0 %) of the people assessed in the test fell into 6 colour codes. Discussion The Japan Colour Research Institute has produced an atlas, “The Medical Colour Standard for skin” with over 500 colour chips mounted on strips of transparent plastic covering a limited range of hues and having the chips more closely spaced for saturation and lightness than in the Munsell system. Having a Nigerian skin colour code has potential usefulness regarding diagnosis (e.g. tuberculosis as discussed above) although the practicality of these is yet to be assessed. It is however likely to be of greater use in monitoring of skin diseases e.g. Vitiligo -noting deterioration or improvement in the patches by colour coding where and when photography may not be readily available. It can be used to assess the changes (objectively) in those who had abused skin lightning /toning creams containing Hydroquinone or corticosteroid. It can be used as an epidemiological tool. There are much variations in the skin colours of Blacks. Ayo Vaughan-Richards [5] in her book Black and Beautiful referred to “the brown red tone of a Ghanaian woman, bronze tone of a Sierra Leonean woman, ivory tone of a Black British woman, honey tone of an Eastern Nigerian woman, yellow –brown tone of an Azanian woman and the blue-black tone of a Kenyan woman”. In a multiethnic/multi tribal nation like Nigeria one sees skin colour variations as well; from the very light complexion of nomadic Fulani in the northern part of Nigeria to the dark complexioned Kanuris in the north-eastern part. The eastern region of Nigeria probably has the second highest prevalence of Albinism in the world - the Cuna Indians of San Blas Island in Panama have about 1-7 /100 inhabitants [6]. The relationship of the colour variation to cutaneous and non -cutaneous diseases will be more relevant with better ways of documentation of skin colour in the West African sub-region. The advantage of this skin colour code is the practicality. Many methods used for skin colour assessment are either too cumbersome or require costly equipments that will not be affordable in developing countries like Nigeria. A second advantage for this format of colour coding is the ease of production. It can be reproduced on almost all the currently available personal computers using the data provided for the various colours – for uniformity /standardization (table 1). The potential problem has to do with the ink /toner used on the colour printers. Where the ink has been spent, used for much work earlier on, and with greater demand on relevant colours, the final product may not match the effect from another printer i.e. there may be slight variations. The ideal proposition of course is for mass productivity production by a few companies using some initially produced cards for standardization similar to what is done for colour photography reprints and in the paint producing industries. The chart can be laminated using thin transparent plastic film. This will prevent wrinkling as well as possible transmission of microorganisms (in a tropical milieu) from the skin of one References
Copyright 2006 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh06013f1.jpg] [jh06013t2.jpg] [jh06013t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}