 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
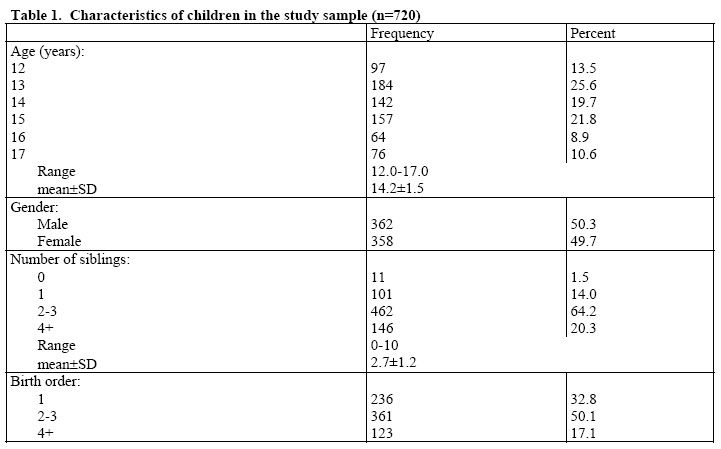
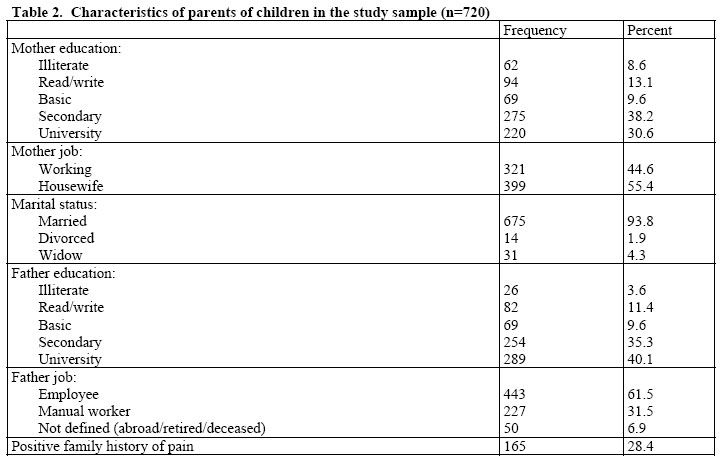
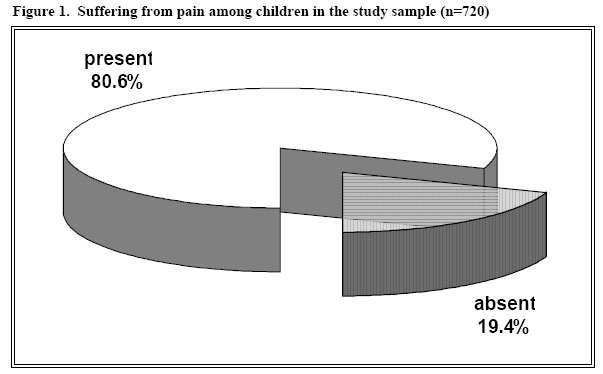
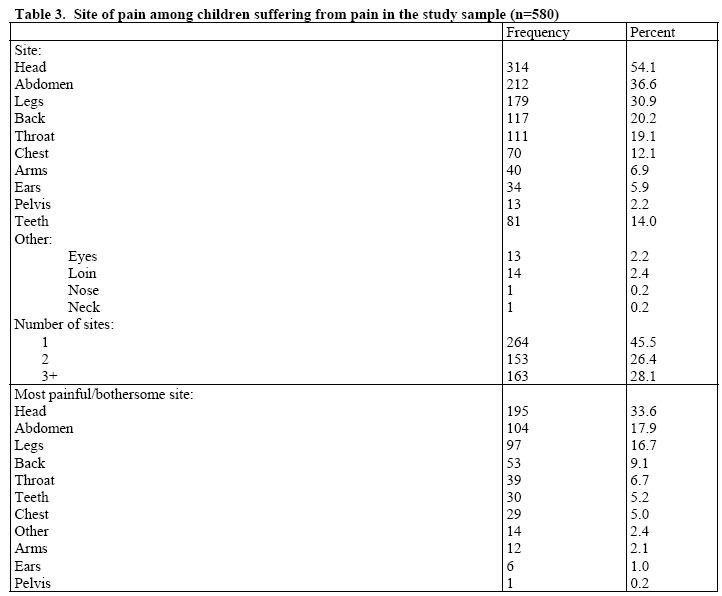
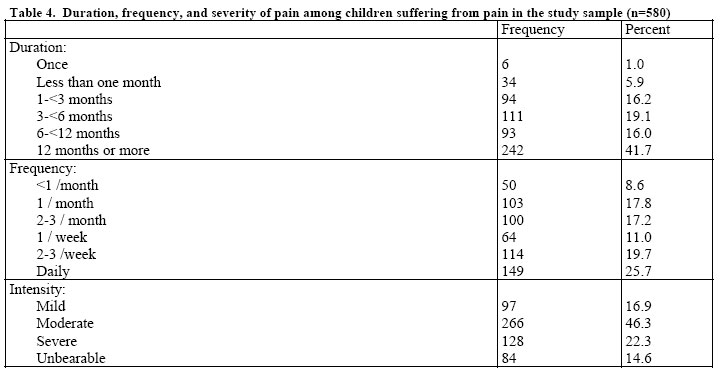
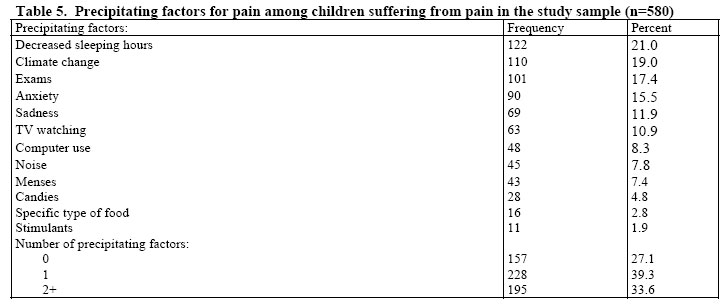
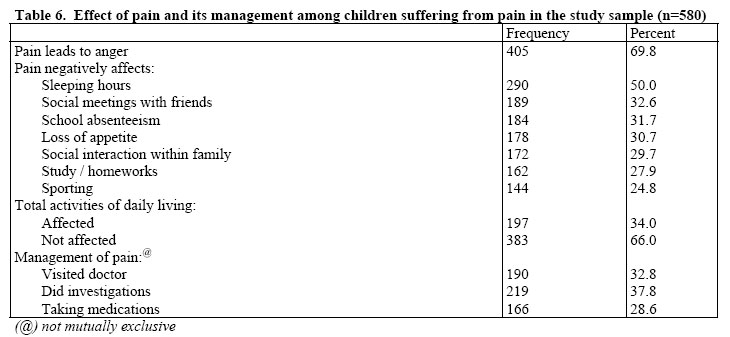
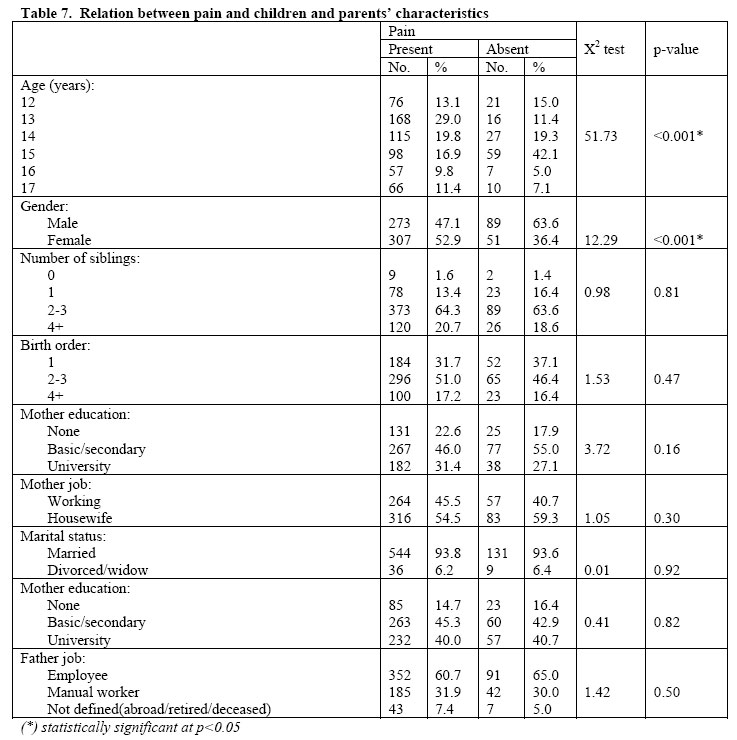
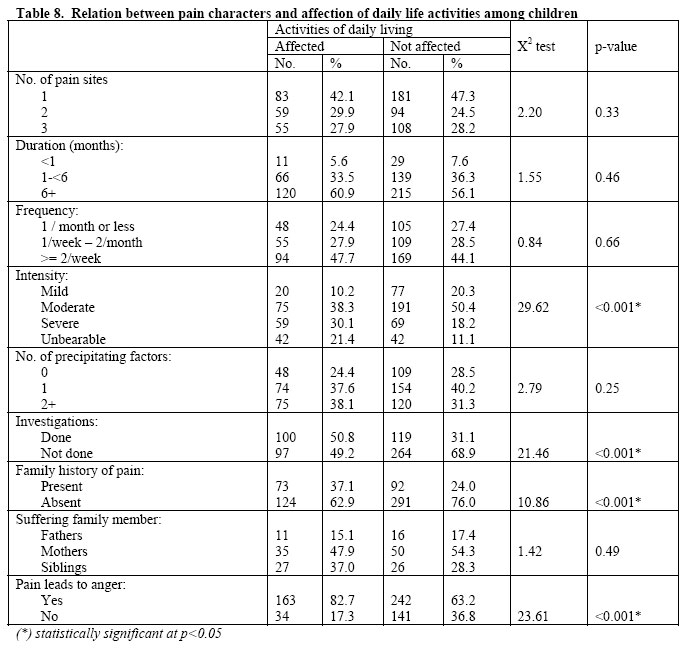
African Journal of Health Sciences, Vol. 13, No. 3-4, July-Dec, 2006, pp. 18-28 Prevalence of perceived pain and its impact on daily lives and activities of adolescents Amal Ahmed Khalil Morsy Faculty of Nursing , Suez Canal University , Orabi and El-Etehad street , Port-Said , Egypt . E-mail: D.Amal_Kh@yahoo.com Code Number: jh06024 SUMMARY Having chronic pain can affect a child’s development in many ways from hindering everyday functioning in family relationships to school and social disruptions. The aim of this study was to investigate the impact of perceived pain on the daily lives and activities of adolescents through measuring the 3-month prevalence of painful conditions, delineating pain features, and describing its consequences. The study was conducted in 4 preparatory and 4 secondary schools in Port-Said city. The 720 adolescent students completed the questionnaire on their own. Of the 720 adolescents, 580 (80.6%) had experienced pain during the preceding 3 months. Headache (54.1%), abdominal pain (36.6%), leg pain (30.9%), and back pain (20.2%) were the most prevalent types. Adolescents with pain reported that their pain negatively affected their sleep (50.0%), social meetings with friends (32.6%), school absenteeism (31.7%), and loss of appetite (30.7%). 41.7% of the adolescents stated that pain had been present for 12 months or more and 46.3% of them reported that their pain was moderate in intensity, while 22.3% reported that it was severe. Also, 32.8% of adolescents visited doctors and 37.8% did investigations for pain. The prevalence of pain was significantly higher among girls than among boys, p<0.001. Activities of daily living were statistically significantly more affected with increasing pain intensity, p<0.001. These study findings would increase knowledge about adolescents’ pain to enable parents, teachers, nurses, and health care professionals to assist young people with pain management, allowing them to intervene positively in their conditions before they become recurrent or persistent. Introduction Chronic pain is a significant problem in the pediatric population. Adolescents and their families experience significant emotional and social consequences as a result of pain and disability. The financial costs of childhood pain may also be significant in terms of healthcare utilization as well as other indirect costs such as lost wages due to time off work to care for the child. In addition, the physical and psychological sequelae associated with chronic pain may have their impact on the overall health, and may predispose to development of adult chronic pain [1,2]. Chronic pain in children is the result of a dynamic integration of biological processes, psychological factors, and socio-cultural context, considered within a developmental trajectory. This category of pain includes persistent (ongoing) and recurrent (episodic) pain, with possible fluctuations in severity, quality, regularity and predictability. Chronic pain can occur in single or multiple body regions, and can involve single or multiple organ systems. Examples of chronic pain include recurrent headaches, abdominal pain, or limb pain [3]. The nursing definition of pain is whatever bodily hurt the patient reports existing, whenever the patient says it does. The cardinal rule in the care of patients with pain is that all pain is real, even if its cause is unknown. Therefore, validation of the existence of pain is based simply on the patient’s report that it exists. This definition is based on two important points. First, the nurse believes patients when they indicate that they have pain. Thus, pain is considered real even if no physical cause or origin can be identified. The second point to keep in mind is that what the patient says about pain is not limited to verbal statements. Nurses encounter patients in pain in a variety of settings, including acute care, outpatient, schools and long-term care settings, as well as the home. Thus they must have the knowledge and skills to assess pain and its effects on the patient, to implement pain relief strategies, and to evaluate the effectiveness of these strategies, regardless of the setting [4]. The pediatric nurse works as a key member of the healthcare team. Her role is to provide education to the adolescent and his/her family about pain disorders and pain management, and to help them with questions or concerns that arise during treatment [5,6]. The evaluation of a child with chronic pain should begin with a history of the current problem, including a careful description of the pain. This should involve detailing the sensory characteristics, intensity, quality, location, duration, variability and alleviating factors. It should also assess the impact of pain on daily life, e.g., sleeping, eating, school, social and physical activities, as well as family and peer interactions [7,8]. Aim of the study This study is aimed at investigating the impact of perceived pain on the daily lives activities of adolescents. This would be attained through 1) documenting the 3-month prevalence of painful conditions among children and adolescents in schools, describing the features of those conditions in terms of location, intensity, frequency and duration, and describing their consequences in terms of restrictions of activities and healthcare utilization. Materials and Methods Setting: the study was conducted in eight schools in Port Said city. These included four preparatory schools (two for boys and two for girls), and four secondary schools (two for boys and two for girls). Sample: this consisted of a stratified cluster random sample, which comprised 720 children aged 12-17 years. The schools were stratified into four strata, according to educational phase, whether preparatory or secondary, and gender, whether boys or girls. Two schools were randomly selected from each of the four strata, for a total sample of eight schools. Within the selected schools, classes constituted the clusters. Two or three clusters were randomly selected from each selected school to fulfill the required sample size. This was calculated to estimate the prevalence of any pain condition of 20% or more, with a 3.0% absolute precision and a 95% level of confidence, using the single proportion equation for dichotomous variables [9]. The required sample size turned to be 683 subjects. After adjustment for a dropout rate of 5%, it was increased to 720. Data collection tools: two tools were used in this study, a self- administered questionnaire form, and a pain questionnaire. The form was developed by the researchers and used to collect biosocial data about adolescent’s age, sex, school grade, residence, number of siblings and birth order. It also included questions about the level of education, occupation and current marital status of the adolescent’s parents. The pain questionnaire was designed to evaluate the prevalence of pain in the preceding three months. Chronic pain was defined as any prolonged pain that lasted a minimum of three months or any pain that recurred throughout a minimal period of three months, at least. The location, frequency, intensity, and duration of pain were addressed by the questionnaire. Choices for pain location were head, back, abdomen, arm, leg, ear, throat, chest, pelvis, tooth, or other. For pain that was described as the main discomfort, the participants were asked to specify the duration, frequency and intensity of the pain. Pain intensity was assessed with the Word-Graphic rating scales [10]. In addition, the questionnaire described the consequences of pain among adolescents in the form of restrictions of daily life activities, as well as healthcare utilization. The type and extent of personal impairment attributable to pain were assessed in the areas of sleep, eating, missed school days, hobbies, social contacts and healthcare utilization in terms of doctor’s visits and pain medication. The participants were asked to rate the impact of the pain in these areas as “yes”, “sometimes” or “no.” Moreover, they were asked whether they had a medical diagnosis for their pain. Furthermore, the participants were asked whether a family member experienced recurrent or chronic pain. Lastly, they were asked whether they became worried due to this pain or not. Pilot study: a pilot study was carried out on a sample of adolescents of different ages in a school other than the selected ones. Their number was 70, about 10% of the main study sample size. Needed modifications were done in the form of re-phrasing and/or omission of some items. The pilot also helped to estimate the time needed for filling the questionnaire forms. Subjects included in the pilot were not included in the main study. Methods: the required official steps were taken to get the approval of carrying out the study from the local directorate of education. Letters were issued to headmasters of selected schools asking indicating the agreement of the directorate to conduct the study, and asking for cooperation with the researcher. Meetings were held with individual headmasters, where the researcher explained the purpose of the study. Oral consents were obtained before any student participated in the study. Ethical considerations were taken into account, and professional advice was provided to any affected student, whenever needed. The students were first surveyed with the pain questionnaire. If the answer to the first question asking about the experience of pain within the past three months was no, then no other questions needed to be answered. Children who reported pain within the preceding three months were asked to continue the questionnaire. The field work was carried out during March 2005. Results The socio-demographic characteristics of the studied children are illustrated in Table 1. It shows that the age ranged between 12 and 17 years, with a mean 14.2±1.5 years. Slightly more than half of the children (50.3%) were males. Nearly one third of them (32.8%) were first born, while 17.1% were fourth or more in birth order. The number of siblings ranged between none (zero) and ten. As shown in Table 2, the highest percentage of mothers (38.2 %) had secondary education, and more than half of them (55.4%) were housewives. Meanwhile, the highest percentage of the fathers (40.1%) had completed university education, and only 3.6% of them were illiterate. They were mostly employees (61.5%). Family history of pain was present among 28.4% of the children. The majority of studied children reported having suffered from pain within the last three months. As Figure 1 displays, such pain was present among 80.6% of children in the study sample. Table 3 indicates that the most common pain sites reported by studied children were the head, abdomen, legs, back and throat. The 3-month prevalence rate of pain in these sites was respectively 54.1%, 36.6%, 30.9%, 20.2%, and 19.1%. In slightly less than half of the sample (45.5%), pain was reported in only one location. Meanwhile, 28.1% of the children complained of pain in three or more locations. When the studied children were asked about the most bothersome pain, headache was at the top of the list (33.6%), followed by abdominal pain (17.9%), and pain in the legs (16.7%). The duration, frequency, and intensity of pain among adolescents suffering from pain in the study sample are displayed in Table 4. The duration was mostly (41.7%) 12 months or more. As for the frequency of pain occurrence, about one fourth (25.7 %) of children reported daily pain episodes. At the other extreme, 17.8% of the children stated that their pain occurred only once per month. Concerning the intensity of pain, it was moderate in the highest percentage of children (46.3%). Meanwhile, 22.3% of them reported their pain was severe and it was unbearable among 14.6%. As for the precipitating factors for pain, decreased sleeping hours was most commonly mentioned (21.0%), followed by climate changes (19.0%), and exams (17.4%). The least mentioned factors were specific types of food and certain stimulants, 2.8% and 1.9%, respectively. As Table 5 indicates, about one fourth of the subjects (27.1%) had no such precipitating factors, while about one third (33.6%) had two or more. The effects of pain were also investigated. Table 6 shows that it led to anger in more than two thirds of the children (69.8%). Moreover, half of them (50.0%) reported sleep disturbances attributable to pain, and in about one third (32.6%) pain prevented them from social meetings with friends. Other effects included loss of appetite (30.7%), absence from school (31.7%), and inability to study (27.9%). Overall, the total activities of daily living were affected by pain among about one third of the participants (34.0%). As for management of pain, about one third have visited doctors for pain (32.8%). Meanwhile, less than one third (28.6%) had taken medications, while more than one third (37.8%) did investigations for pain. The relation between pain and children and parents’ characteristics has revealed two statistically significant associations, namely with child age (p<0.001), and gender (p<0.001). As Table 7 illustrates, the percentage of children having pain was highest at the ages of 13 and 14 years (29.0% and 19.8%, respectively), while it was mostly absent at the age of 15 years (42.1%). Also, the table shows more females suffered from pain, compared to males (52.9% and 36.4%, respectively). Regarding the relation between pain characters and affection of daily life activities, Table 8 points to statistically significant association with pain intensity (p<0.001), having done investigations (p<0.001), family history of pain (p<0.001), and pain leading to anger (p<0.001). As the table demonstrates, daily life activities were affected with the increase of pain intensity, and was associated with a higher percentage of doing investigations (50.8%), more family history (37.1%), and more anger (82.7%). Discussion Children and adolescents frequently experience pain. The 3-month prevalence of pain in the present study was 80.6%. A close figure was reported in a previous study where out of the 749 children and adolescents, 622 (83%) had experienced pain during the preceding 3 months [11]. Headache is the most common pain disorder among children and adolescents [12]. An important finding of the present study was that headache was the most bothersome pain, as reported by participants. This might be attributed to the fact that headache would have a negative effect on all types of activities of daily living. According to the study, in one third of the studied children, pain affected their total activities of daily living. This interpretation is in line with another study that found that recurrent headaches have an impact on child’s life in a number of ways, including school absences and reduction in performance, decreased home and family interactions, and decreased socialization with peers [13]. Abdominal pain was the second most bothersome pain reported by studied children. This result is in agreement with another study that has similarly reported that more than one third of children complained of abdominal pain lasting two weeks or longer [4]. On the same line, it has been mentioned that recurrent abdominal pain is a common reason for children to see a doctor. About one third of studied children in the present work have visited a doctor for pain [15]. Regarding pain in legs, the results of the present study showed that this type of pain was the third most bothersome pain as reported by studied children. This might be interpreted by the large number of children and adolescents practicing sports and games at this age, which might be associated with minor or moderate types of musculo-skeletal pain. This view is in congruence with the “Keep Kids Healthy” study, where it was mentioned that it is very common for children to complain of knee pain, especially adolescents that are active in sports [16]. According to the present study findings, back pain was the fourth bothersome pain type, and also the fourth in its frequency of occurrence, being reported by about one fifth of participants. This pain might be attributed to high level of physical activity at this age, in addition to the commonly mentioned factor of carrying heavy backpacks. In this regard, it has been reported that the prevalence of nonspecific back pain increases dramatically during adolescence from less than 10% in preteens up to 50% in 15-16 years olds. Also, statistically significant associations were found between back pain and backpack use, female gender, body mass index, general health, physical functioning and bodily pain [17]. Meanwhile, British researchers have studied the prevalence of low back pain in school-age children and the factors that increased a child’s risk for back pain. Their results have indicated that the physical stress of carrying a heavy backpack is not a major cause of childhood back pain. Children with emotional difficulties or who participated in sports were more likely to complain of back pain [18]. Nearly one third of the present study participants who had pain visited doctors and were taking medications for pain. This is supported by the finding that about one third were complaining of severe and unbearable pain, which would force them to visit a doctor and take medications to relieve this pain. In this respect, it has been suggested that health care utilization because of pain varied according to pain location. Children and adolescents with abdominal, limb and/or back pain more often reported visiting a doctor than did those with headache [19]. In contrast, children and adolescents with headache most often reported taking medication for their pain. In accordance with these results, the use of medications among 50% of children with persistent or recurrent headaches or migraines has also been reported [20]. The most frequent triggers for pain perceived by participants in the present study were lack of sleep and daytime sleepiness, climate changes, examinations, anxiety, sadness and length of exposure to media such as television and computers. These results are in accordance with a study that found that 12.8% of participants reported that their pain was triggered by television or computer use and 16.2% by lack of sleep. Similar proportions of children and adolescents perceived psychological factors as triggers of pain [21]. The present study was also aiming at documenting the impact of pain experienced by children and adolescents. More than one third of the respondents reported restrictions of total activities of daily living resulting from pain. Half of the participants have reported sleep disturbances attributable to pain. This is in agreement with a study that has also added that sleep disturbances among children affect many areas of their lives, including school attendance and performance, emotional state and relationships with family members and friends. Moreover, sleep disorders with frequent nocturnal arousals or daytime somnolence are common among children suffering from chronic headaches, migraines or juvenile rheumatoid arthritis [22]. Furthermore, pain may have a negative effect by interfering with sleep and thereby hampering recovery from an acute illness or decreasing appetite [4]. This might also explain the high percentages of school absenteeism and/or problems with school activities. In the present study, about one third of participants reported school absenteeism attributable to pain. Restrictions on maintaining social contacts and activities with same age friends are other important signs of chronic and recurrent pain conditions. In the present study, about one third of respondents reported not being able to socialize with their friends due to pain. This is in congruence with what had been emphasized that chronic pain may affect the person’s quality of life by interfering with work or interpersonal relationships [4]. According to the present study findings, there was a statistically significant association between the presence of pain and age. The frequency of pain was found to peak at the age of 13 years. This can be attributed to the fact that early adolescence begins from age 10 to 13 years, and there are physical and physiological changes during this period, which may be accompanied with pain. In this regard, it has been stated that early adolescence, with the onset of puberty and physical and psychological changes, involves a great deal of stress and pain for children and families [23]. Also, in the present study, pain turned to be statistically significantly higher in females, compared to males. This can be attributed to the fact that a considerable proportion of the precipitating factors for pain is menses, which may increase the prevalence of pain among girls than boys. Moreover, pain in children is multidimensional and is affected by gender, genetic variations, emotional status, temperament, developmental level, culture and ethnicity, and previous parental response to the child’s pain [24,25]. Investigations done were significantly high when the activities of daily living were affected, as revealed from the present study findings. On the same line, it has been reported that fear and frustration are often fuelled by unhelpful or inaccurate diagnosis such as functional or psychosomatic pain. Families often interpret these labels as blaming them for the child's pain, and the labels tend to reinforce their need to move from doctor to doctor in search for a different diagnosis and cure [26]. Also, pain leading to anger was statistically significantly higher when the activities of daily living were more affected. These present study results are in agreement with what has been reported that pain for an extended period of time often results in disability. Patients with a number of chronic pain syndromes report depression, anger and fatigue. They also score lower on quality of life measures [27, 28]. Recommendations In view of the foregoing findings, the following recommendations are proposed.
To help reduce the negative impact that chronic pain has on a child’s life, it is important that families seek psychological services as part of the treatment approach to their child’s pain problems. Further studies are necessary and may enhance our knowledge about pediatric pain to enable parents, teachers and health care professionals to assist young people with pain management, allowing them to intervene positively with their conditions before they become recurrent or persistent. Conclusion In conclusion, the majority of studied children have reported having suffered from pain within the last three months. The most common pain sites were the head, abdomen, legs, back and throat. The duration was mostly 12 months or more, and the intensity was mostly mild to moderate. Decreased sleeping hours was the most commonly mentioned precipitating factor. The total activities of daily living were affected by pain among about one third of the participants, and about one third have visited doctors for pain. Pain had statistically significant association with child age and gender. Affection of daily life activities increased with pain intensity. References
Copyright 2006 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh06024t2.jpg] [jh06024t1.jpg] [jh06024t7.jpg] [jh06024t5.jpg] [jh06024t6.jpg] [jh06024f1.jpg] [jh06024t4.jpg] [jh06024t8.jpg] [jh06024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}