 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
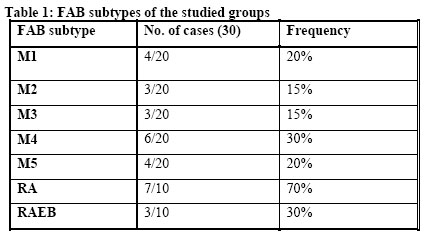
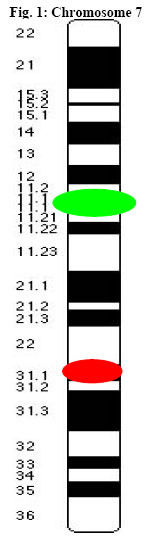
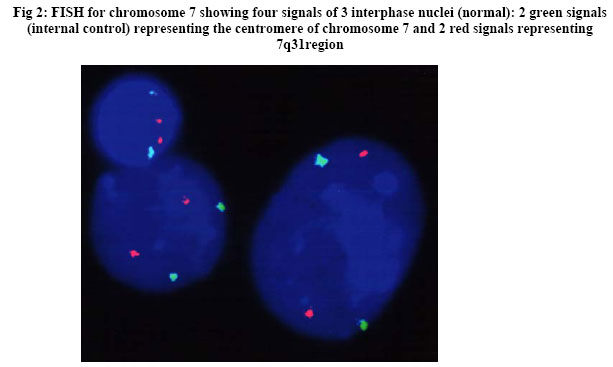
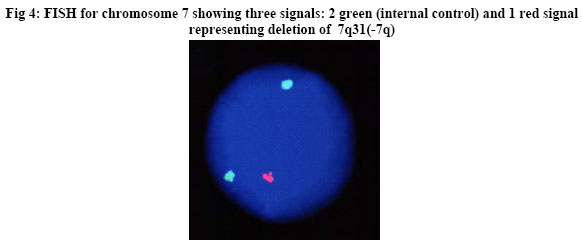
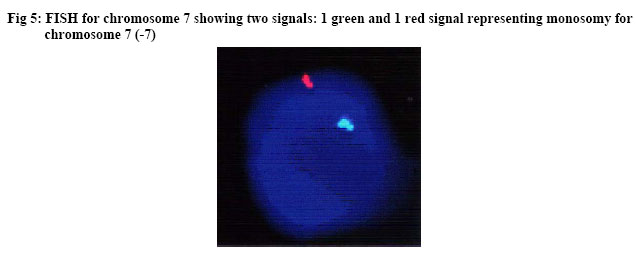
African Journal of Health Sciences, Vol. 13, No. 3-4, July-Dec, 2006, pp. 33-42 Molecular characterization of chromosome 7 in AML and MDS patients Heba N. Abdelrazik*, Hala M. Farawila, Mai A Sherif, Mervat AlAnsary Clinical Pathology Department, Faculty of Medicine Cairo University 14 Aly El Gendy, 6th district Nasr City, Cairo, Egypt *Author for Correspondence: . E-mail: hebanabil@gmail.com Code Number: jh06026 SUMMARY Myelodysplastic syndromes (MDS) share many features with acute myeloid leukemias (AML) and in fact 20 - 40% of the patients eventually develop a picture of full blown AML. Chromosome 7 has been a focus of attention as a site harboring tumor suppressor genes whose loss of function contributes to leukemia transformation or tumor progression. Abnormalities of chromosome 7 are frequently encountered in AML and MDS. The aim of the present study was to detect the molecular abnormalities of chromosome 7 in Egyptian AML and MDS patients using the FISH technique and whether the abnormality has an implication on the prognosis of the disease after a period of one year follow up. Fluorescence in-situ hybridization (FISH) was performed for chromosome 7 using a locus specific probe for 7q31 and a centromeric probe from 7p11.1-q11.1 in a series of 30 patients diagnosed as: AML (20 patients) and MDS (10 patients) according to the FAB criteria. Aberrations of Chromosome 7 were found in 36.6% of AML patients: 3 cases showing monosomy with a mean positivity of 17.3%, 2 cases showing 7q deletion with a mean positivity of 11%. While both monosomy and deletion were detected in 3 cases. However, in MDS patients; monosomy for chromosome 7 was the only abnormality detected and was found in 30% of cases. Genetic abnormality of chromosome 7 showed a significant association with poor prognostic criteria. Patients who had normal FISH results showed a higher percentage (31.6%) of complete remission (CR) versus 0% in patients with monosomy or deletion who showed a higher percentage (100%) of death or poor response to therapy (NR). Although AML patients had a worse prognosis when compared to MDS patients, patients with genetic abnormalities showed the worst outcome. Introduction The long arm of human chromosome 7 between 7q22 and 7q36 has been identified as a region harboring one or more tumor-suppressor genes (TSGs) inactivated in acute myeloid leukemia (AML) [1]. Allelotyping studies have delineated at least three distinct loci that are frequently deleted [2, 3]: 7q22, 7q31.1, and 7q31.3. Among these, a correlation between survival and deletion limits implicates loss in the cytogenetic bands 7q31~q32 in refractoriness to therapy [4, 5]. Complete and interstitial losses of chromosome 7 (-7, 7q-) are nonrandom anomalies seen in de novo and therapy-induced myeloid neoplasms as well as leukemias arising from occupational or environmental exposure to mutagens. Monosomy 7 in adult myeloid neoplasms, is more common than the interstitial deletions of the long arm (7q-). The importance of monosomy 7 is evident from the small but significant number of adult acute myeloid leukemia (AML) cases in which it occurs as the sole anomaly [6]. Childhood monosomy 7 seen secondary to Fanconi’s anemia, juvenile chronic myeloid leukemia, Down’s syndrome as well as familial monosomy 7 may share genetic alterations associated with adult myeloid neoplasms [7]. The poor prognosis associated with chromosome 7 anomalies in adult myelodysplasia (MDS) and AML underscores the need for molecular analysis [8, 9]. Interstitial deletions of 7q, seen in a variety of solid tumors with distinct segments of loss at bands 7q11, 7q22, and 7q31 that are apparently unique to specific neoplasms, have raised the possibility of a number of tumor suppressor genes in the long arm of chromosome 7 [10]. In the past, delineation of the critical regions of loss in 7q has been the focus of several investigations on solid tumors as well as hematopoietic neoplasms [11-13]. Fluorescence in situ hybridization analyses have delineated a critical region of loss at 7q22 in myeloid malignancies [14]. Other studies have raised the possibility of unbalanced translocations of fragments of chromosome 7 being located on marker chromosomes; patients who were perceived to be monosomic by centromere-specific probes showed strong hybridizations to marker chromosomes with chromosome 7-painting probes [15]. However, the extent and variability of 7 q deletions have so far prevented the identification of a putative tumor suppressor gene. The molecular mechanisms underlying these chromosomal abnormalities also remain unclear. Other investigators have identified a number of sequence elements/motifs that are frequently present near the breakpoints of chromosomal rearrangements and may suggest how these rearrangements occurred. They include Alu repeats, chi-like sequences, DNA topoisomerase II consensus binding sites and sequences with homology to the heptamer and nanomer motifs of the V(D)J recognition signal sequence [16]. Accordingly, the present study aimed to detect monosomy 7and 7q31 deletions among AML and MDS patients using FISH probes and to correlate whether the abnormality has an implication on the prognosis or response to therapy. Materials and Methods Patients Forty samples were included in this study. Twenty AML and Ten MDS patients who were newly diagnosed in Al Kasr El-Aini Hospital over a period of 2 years from January 2002 to January 2004 were enrolled in this study. Their ages ranged from 20-65 years with a mean of 41 years and the male to female ratio was 1.1. The diagnosis and sub classification of MDS and AML was based on morphological and cytochemical studies of peripheral blood (PB) smears, bone marrow (BM) aspirates, and biopsy specimens obtained before therapy, and immunophenotyping (Table 1)according to the French-American-British Cooperative Group criteria [17,18]. Ten age matched controls were involved to normalize FISH results. Complete hemogram and biochemical tests were done to the control group before the FISH analysis which was done on PB samples. Immunophenotyping 10ul EDTA blood from each case was mixed with a panel of monoclonals; CD45,34,13,14,33&38 (all purchased from Becton-Dickinson) after RBC’s lysis and processed according to the manufacturer’s guide. Analysis was performed on FACScan (Becton-Dickinson), lymphocytes or blasts were gated on a forward and side scatter profiles (>20% positivity were considered positive) [19]. Culture Fresh peripheral blood PB samples were obtained from the control group and fresh bone marrow samples were used for all 30 MDS and AML cases. Mononuclear cell layer was separated using ficol hypaque density gradient centrifugation from both PB and BM samples [20]. Mononuclear cells were cultured for 24 h (short-term cell culture) without PHA. Five milliliters of RPMI 1640 medium supplemented with 15% of fetal calf serum and 1% L-glutamine were added to each culture tube. The cell concentration in the medium was adjusted to 1x106/ml. Colcemid at a final concentration of 0.05 µg/ml was added 60 min before harvesting. Cells were treated with 0.075 MKCl hypotonic solution at 37°C for 15 min followed by three changes of 3:1 methanol:glacial acetic acid fixative solution. The cells were finally resuspended in this fixative solution. The cells suspended in fixative solution were spread on slides in a Thermotron (CDS-5) at 30°C and 40% of humidity. The slides were put in a 2x SSC ( 1x SSC =150 mM sodium chloride and 15 mM sodium citrate solution) bath at 37°C for 30 min and then dehydrated in 70%, 80% and 100% ethanol. After air-drying the slides, FISH procedures were performed [21]. FISH FISH analysis was performed using the commercially available locus specific identifier, LSI D7S522 Spectrum Orange/ CEP 7 Spectrum Green Dual Colour probe which hybridizes to band 7q31 (Spectrum Orange LSI D7S522) and to the centromere band region 7p11.1-q11.1, locus D7Z1 (Spectrum Green CEP 7) of human chromosome 7 (Vysis, Downers Grove, IL USA) according to the manufacturer’s instructions. Improvements were obtained by incubating bone marrow slides at room temperature overnight before digestion with proteinase K (stock solution 1mg/ml) for 6 min at 37°C. After washing twice with phosphate buffer solution lx, slides were fixed in a 1% formaldehyde solution; they were then denatured in 70% deionized formamide/2xSSC solution for 5 min at 74°C then successively passed through70%,80% and 100% ethanol at -20°C. The probe was denatured at 74°C for 5 min and added onto the slide and then covered with a coverslip. Hybridization was performed overnight at 37°C in a humidified chamber. Post-hybridization washing was done in 4xSSC NP 40 for 2 min at 74°C first and then for 2 min at room temperature. Slides were counterstained and mounted with DAPI II. Image analysis and scoring Images were viewed under the fluorescent microscope with the proper filter set: DAPI /orange/green were used to visualize the fluorescent signals. A total of 500 interphase and metaphase nuclei were analyzed using Vysis scoring criteria blindly scored by two individuals for each sample. The pictures were captured by using an Olympus BX60 microscope equipped with compulog IMAC-CCD S30 camera module and the insitu imaging system (ISIS 2) software version 2.5 (MetaSystem, Belmont, MA,USA). using x 100 objective lens. The centromere appeared as a green signal while 7q31 appeared as an orange signal. The number of fluorescent signals for each nucleus was noted as: 4 signals: 2 green and 2 orange were counted as a normal cell. 3 signals: 1 orange and 2 green indicated deletion (7q-). 2 signals: 1 green and 1 orange indicated monosomy 7 (-7) 0 (no signal could be seen): failure of hybridization, excluded Split signal: 2 signals with very short distance in-between were counted as 1 signal. Occasionally the probe may appear as five to six signals depending on the condensation of the DNA and relative distance between chromatids. The signals may appear diffuse or split. In normal metaphase, LSI D7S522 may appear as 1 to 2 signals on each chromosome 7. Normal control specimens were incorporated and the cut off level was evaluated at 5 % [22,23]. Results The 40 cases were classified into 3 groups: Group A; 20 AML patients, Group B; 10 MDS patients (Table 1) and Group C; 10 normal age-matched controls. Cytogenetic studies Chromosome 7 abnormalities were detected in 36.6% (11/30) of the patients. Eight patients were AML and 3 patients were diagnosed as MDS, Table 2 summarizes the type of abnormality detected in each group. Association between the clinical, hematological data and the cytogenetic study A higher predominance of females; 9 females versus 2 males, was found in patients with chromosome 7 anomaly and the difference was statistically significant (P=0.02). The anomalies were also associated with splenomegaly and lymphadenopathy (P-value 0.034 and 0.043 respectively). Moreover, patients with Chromosome 7 abnormality showed a significantly higher mean TLC and PB blast cell counts (P=0.03 and 0.01 respectively). Of the 8 AML cases showing chromosome 7 abnormality, 3/6 (50%) cases were M4 phenotype, 3/4 (75%) cases were M5 phenotype while 1/4 (25%) case was M1 and 1/3 (33%) case was M2. While the 3 monosomic MDS cases were Refractory anemia with excess blasts (RAEB) (none was refractory anemia [RA]). However there was no significant association between the type of leukemia and the chromosomal abnormality (data not shown). Association between the clinical oqutcome and the cytogenetic study Patients were followed up for a period of one year, 6 patients entered in complete remission (CR), (BM. samples were morphologically and immunophenotypically normal). MDS patients who turned to AML and AML patients who relapsed or failed to enter in complete remission were considered non responders to therapy (NR), these were 17 patients [21]. Patients who died due to relapse, organ failure or therapy related mortality were considered “Died”, and they were 7 patients. Patients who had normal FISH results showed a higher percentage of complete remission CR while patients with monosomy or deletion had higher rates of death or showed no response to therapy (NR) (p = 0.03) (Fig 6) FISH results were also interpreted quantitatively; the number of positive nuclei was counted. These results also revealed a worse prognosis towards those who had a higher percentage of the genetic abnormality and the p-value was 0.027 (Table 3). Comparison between AML and MDS On comparing AML with MDS cases regarding the outcome, AML patients had a worse outcome (P =0.03) (Table 4). Comparison between MDS and AML patients with the anomalies was not done due to the low number of MDS patients having chromosome 7 anomaly (3 cases) and they were all monosomic. Discussion The association between losses in the 7q region and the appearance of myeloid leukemia suggests that this region contains tumor suppressor gene(s) whose loss of function contributes to leukemia transformation or tumor progression but definitive evidence for their role has not been yet established. [11,24]. The complexity of 7q rearrangements suggests that a synergy of different genetic factors, rather than the alteration of a single tumor suppressor gene, could be involved in the pathogenesis of del (7q) in myeloid disorders [25]. On the basis of cytogenetic and molecular methods, several critical regions in 7q have been identified in chromosome bands: 7q22, 7q31.1, 7q32, 7q33-34 and 7q35-36 [26]. Aberrations of chromosome 7 are usually difficult to determine because of the heterogeneity of breakpoints and their occurrence in complex karyotypes, which are difficult to analyze cytogenetically. Complex karyotypes with multiple unbalanced translocations are observed in most cases of AML with –7/7q-. Thus, in many cases, fluorescent in situ hybridization (FISH) analysis may be helpful in revealing the involvement of this chromosome in structural aberrations. Taking into consideration the sensitivity of this technique, it can also confirm the numerical aberrations of chromosome 7, even when they occur in small populations of cells. Since –7/7q- aberrations are considered as a poor prognostic factor in malignant myeloid disorders, establishing their presence is very important from the clinical point of view [27]. Thus, the aim of the present work was to detect the molecular abnormalities of chromosome 7 (monosomy 7 and 7q del, –7/7q-) in MDS and AML patients using the FISH technique and whether it has an implication on the prognosis of these diseases. Abnormalities of Chromosome 7 were found in 40% of patients in Group A and 33% of patients of Group B. However, the AML group (Group A) revealed both abnormalities, –7/7q- while monosomy 7 (–7) was the only abnormality found in Group B. Similar frequencies were observed by Brozek et al [9] and Chang et al. [28], the latter studied chromosomal abnormalities in 52 primary MDS patients in which abnormalities involving chromosome 7 was the most frequent cytogenetic abnormality and was found in 31% of cases. These were higher than previously observed by other authors, who detected -7/7q- in 12%,8% , 9% , 7.8% of AML patients respectively [29,30,31,32]. Others revealed monosomy 7 in 8% and 7q- in 5% of AML cases [33]. Most of our cells failed to enter in metaphase and the count was carried on interphase cells yielding this relatively high frequency of Chromosome 7 aberrations which according to Brizard et al [34] would have given a lower percentage if metaphase cells were studied. This may also yield discrepancies between results of interphase FISH and conventional cytogenetics (CC) carried on metaphase spreads as detected by Kadam et al [35]. They explained that the aberrant clone are in G0 at the time of examination by CC or the inability to enter mitosis in vitro thereby passing undetected by metaphase examination [36]. They concluded that certain chromosomal aberrations e.g. those involving chromosome 7 are underestimated by Gbanding as a result of 2 factors: a) some cells do not proliferate in culture and hence cannot be karyotyped and b) others give rise to poor morphology metaphases which are excluded from the scoring. Direct evidence for three distinct segments of chromosomal loss in the bands 7q22–31 have been identified [26]. Liang et al [37] found that more than 80% of their AML cases revealed allele loss for the entire region, a rare case of the 7q-chromosome showed allele loss for only the proximal 7q31.1 loci flanked by the markers D7S486 and D7S2456. Also, one of their cases with monosomy 7 revealed allele loss for loci at both 7q31 and 7q22 with retention of sequences between these sets of loci. Furthermore, a case of AML with no cytogenetic anomaly of chromosome 7 revealed a submicroscopic allelic imbalance for a third distal locus, D7S677. These findings suggest the presence of three distinct critical loci that may contribute alone or in combination to the evolution of MDS and AML. The data also provide molecular evidence for unbalanced translocation with noncontiguous deletions, as an alternate mechanism underlying monosomy 7. This may also suggest that some of our patients may have had abnormalities in chromosome 7 outside 7q31 with intact chromosome 7 centromere, thus giving false normal results which reflects an underestimation of the frequency of the anomaly Monosomy of chromosome 7 was detected in 6 of our patients (3MDS and 3AML) with a mean FISH positivity of 17.3% and 7q deletion was detected in 2 cases (AML) with a mean positivity of 11% while both monosomy and deletion were detected in 3 cases of the whole studied group as shown in Table 2. These 3 cases were 2 males and 1 female, 2 of which had splenomegaly, hepatomegaly and lymphadenopathy. All of them had monocytic leukemias and none showed CR (2 of them died and 1 showed NR). There was a significant association between the presence of splenomegaly, lymphadenopathy, high TLC and peripheral blood (PB) Blast cell count with the presence of genetic anomaly, indicating the poor prognostic nature of chromosome 7 anomalies [38] Aneuploidy of chromosome 7 was more frequently or the sole abnormality encountered in our MDS cases especially in the refractory anemia with excess blasts (RAEB) FAB subtype. Chromosome 7 aberrations were not encountered in M3 FAB subtype cases, in contrast to M4 and M5 cases in which they were frequently encountered. This may be attributed to the less favorable prognosis of M5 with extramedullary infiltration; gum infiltration and CNS disease [39]. Patients who had normal FISH results (19 patients) showed a higher percentage (31.6%) of complete remission (CR) versus 0% in patients with monosomy or deletion (11 patients) who never entered in CR (100%) and either died or showed no response to therapy (NR). Similar data were reported by other authors [9,11]. In the study by Brozek et al only 21% of patients with these abnormalities reached complete remission, showing a bad prognosis and poor response to therapy in the group of -7/7q- patients [9]. Quantitative FISH results also revealed a worse prognosis towards those who had a higher percentage of genetic abnormality. AML patients had a worse outcome when compared to MDS patients. This is obvious from the pathogenesis of both diseases where in AML the normal marrow elements are replaced sometimes totally by the malignant blasts, whereas in MDS, there is insufficient differentiation capacity of the progenitors to mature blood cells [40]. Clinically, malignant myeloid disorders exhibiting -7/7q- have been associated with bad prognosis with high susceptibility to infections, poor response to chemotherapy, and short survival times [11,41]. Studies demonstrated that FISH provides a rapid, quantitative method for the detection of cells with chromosome abnormalities in peripheral blood and bone marrow specimens. FISH could detect MRD in specimens that seemed normal by all standard morphological and cytogenetic criteria. Since FISH can be applied to interphase cells, results can be representative of the entire populations rather than restricted to cycling cells as is the case with routine cytogenetic analysis. Furthermore, the hybridization time will allow pretreatment investigations and disease monitoring to be performed directly on bone marrow smears with results available on the day of specimen collection. Also, the small amount of material required for FISH examination is particularly useful in hypocellular marrows and when aspiration is difficult [42]. Chromosome 7 abnormalities are heterogenous and some are part of unexpected complex rearrangements often impossible to detect or interpret correctly without using FISH techniques. Also, deletions may be accompanied by translocations which are identifiable only by FISH [43]. Diagnostic accuracy in acute leukemias can be improved if traditional morphology and cytochemsitry are supplemented with immunophenotyping and genotypic analysis. This multiparameter approach is of crucial importance for the management of patients as it enables the identification of leukemic syndromes with distinct biological features and response to treatment. Cytogenetic findings can be quite helpful in establishing the correct diagnosis and can add information of prognostic significance [44]. They help in the diagnosis, prognosis, monitoring and therapy decisions [32]. Conclusion While FISH will not replace routine karyotypic analysis of material at presentation, it does provide a powerful and sensitive tool for monitoring the disease in patients with karyotypic abnormalities. Thus the detection of chromosome 7 abnormalities by FISH is very important since this chromosome harbors tumor suppressor genes so this allows better understanding of the mechanism of leukemogenesis and the molecular categorization of these diseases for better stratification of treatment modalities. References
Copyright 2006 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh06026t4.jpg] [jh06026t3.jpg] [jh06026t1.jpg] [jh06026f2.jpg] [jh06026t2.jpg] [jh06026f4.jpg] [jh06026f3.jpg] [jh06026f6.jpg] [jh06026f1.jpg] [jh06026f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}