 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
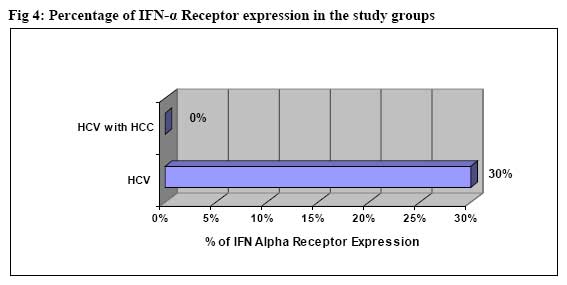
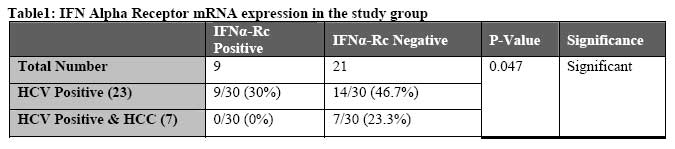
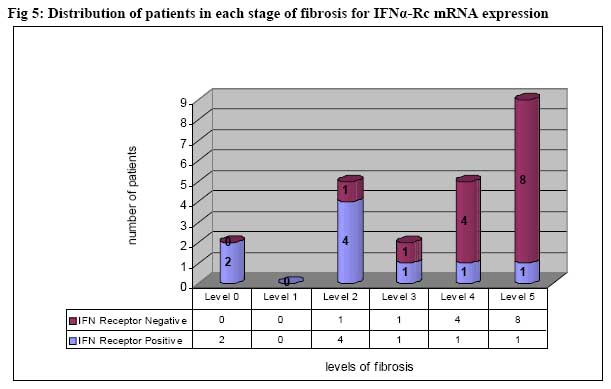
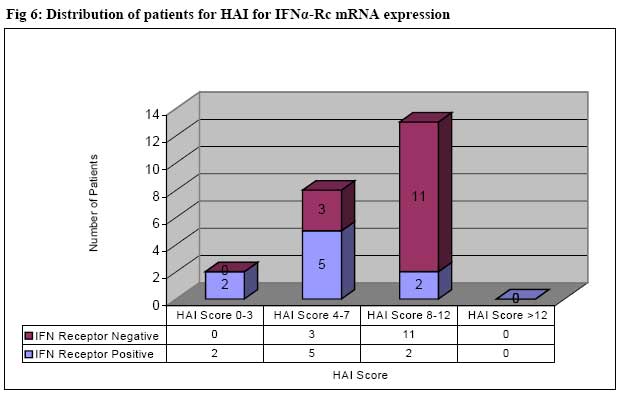
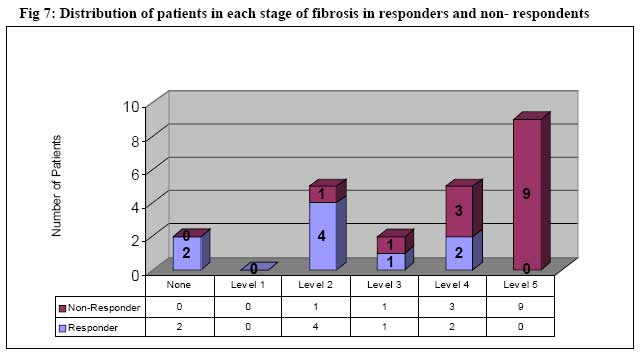
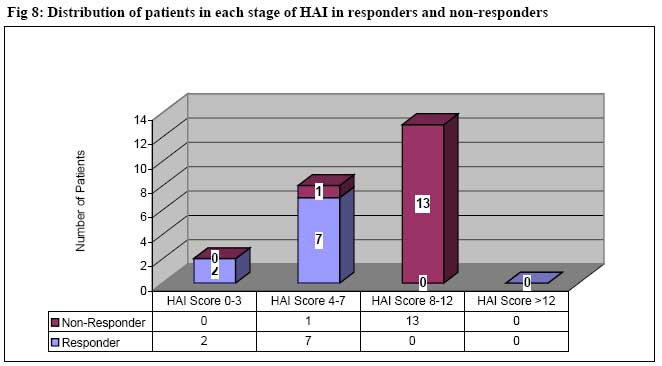
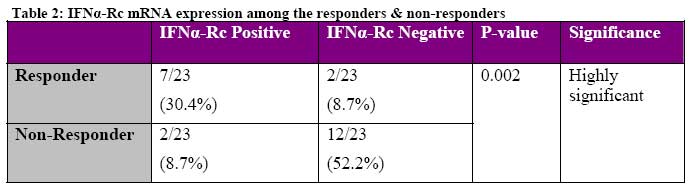
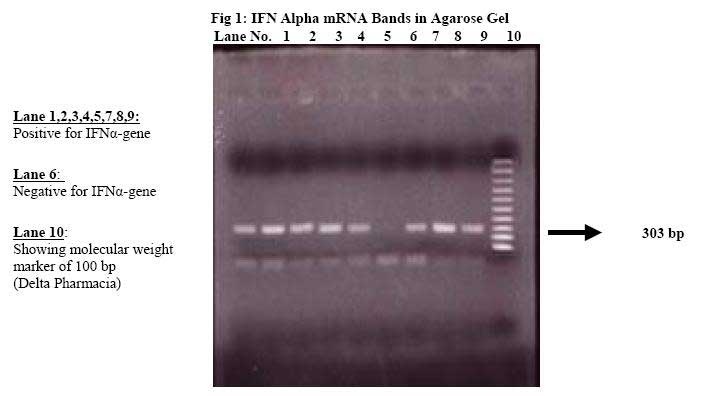
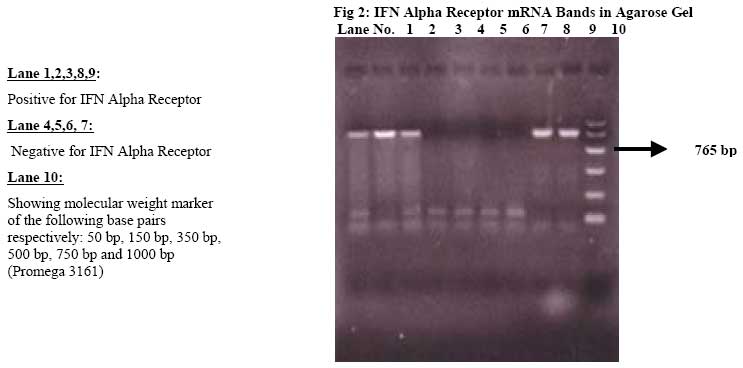
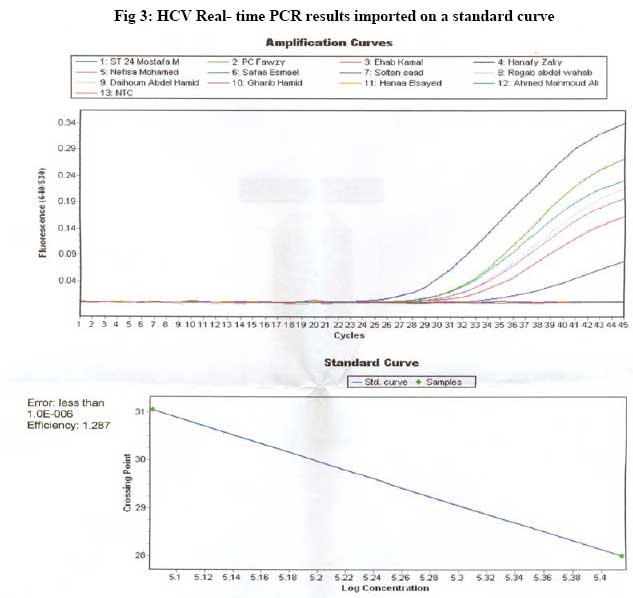
African Journal of Health Sciences, Vol. 14, No. 1-2, Jan-June, 2007, pp. 86-96 Intrahepatic expression of interferon alpha & interferon alpha receptor m-RNA can be used as predictors to interferon response in HCV and HCC patientsHosni Salama¹, Hazem Ali Atta², Heba Abdelrazik³* 1. Department of Tropical Medicine- Biochemistry; 2. Department of Clinical Pathology; 3. Faculty of Medicine, Cairo University Code Number: jh07012 SUMMARYChronic hepatitis C Virus (HCV) is the leading cause of liver cirrhosis worldwide and in Egypt. Patients with cirrhosis secondary to chronic HCV infection are at increased risk for developing Hepatocellular carcinoma (HCC) in which Interferon therapy is the only effective anti-viral therapy. The current study aimed to investigate the expression IFN-αand IFN-αReceptor genes in liver biopsies from patients with HCV and HCC. Correlation of their expression with the clinical, histopathological progress of the disease and the effectiveness of IFN therapy in HCV patients after a period of 6 months follow-up was done. Expression of IFN-α and IFNα-Rc m-RNA was investigated by RT-PCR using liver biopsy specimens from 30 HCV patients including 7 patients complicated with HCC. Liver biopsies were also subjected to formalin fixation for complete histopathological examination. Ninety seven percent of patients expressed Interferon Alpha m-RNA while 30% only expressed Interferon Alpha Receptor m-RNA. Responders and non-responders to Interferon therapy were divided according to their HCV RNA after six-months follow up period of interferon therapy. Responders showed significantly lower mean age, better histopathological states and higher incidence of expression of IFN Alpha Receptor mRNA. Regardless of the response to interferon, histological activity index scores and the degree of fibrosis showed a significant inverse correlation to the presence of IFNα-R m-RNA. IFNα-R mRNA expression decreases with the histological progress of the disease, suggesting that lower expression of the IFNα-Rc may be partially responsible for the unfavorable response to interferon in these patients. Introduction Interferon therapy is the only strategy at present potentially capable of eliminating HCV from hepatocytes [1]. However less than half of Egyptian HCV patients are able to eliminate HCV RNA from their serum with IFN therapy and most relapse after cessation of therapy [2]. Persistent HCV infection is a major risk factor for the development of HCC. Approximately 80% of Japanese HCC patients are also diagnosed with HCV-associated cirrhosis or chronic hepatitis C. It has also been shown that the risk of HCC increases with the degree of liver fibrosis [1]. HCV-related end-stage liver disease is now the principal indication for liver transplantation in Egypt [3]. Almost all viruses, however, have evolved mechanisms to evade the interferon system by partially blocking interferon synthesis or interferon action. Viral evasion mechanisms include block of interferon synthesis, blocking of interferon signaling, and blocking of the function of IFNinduced proteins [4]. IFN treatment is expensive and causes severe side effects, thus prediction of response to IFN is especially meaningful for patients with HC and HCC [5]. However, the determination of IFN responsiveness is complicated and several factors may influence it. HCV titre and genotype, heterogeneity of the virus (mutations in NS5A proteins) and interferon sensitivity determining region of the viral genome (ISDR) are all viral related factors [6-8]. Host factors also influence the responsiveness, including younger age, female sex, low pretreatment HCV RNA level, absence of fibrosis or cirrhosis, higher or longer doses of IFN, and non-type 1b viral genotype have been associated with an increased response to IFN-α therapy [9]. IFN-α acts on target cells to confer a state of resistance to viral infectivity at one or more stages of virus entry or replication. These biological effects require binding to the type I IFN receptor complex, which is composed of two subunits, α and β[10]. Synthesis of Interferon is induced by activating the Jak-Stat pathways of cell signaling. The signaling is initiated through the binding of these protein kinases to the Interferon receptors, Type 1 and Type II. IFN-α and IFN-β have a common receptor (Type 1) while IFN-γ has its own receptor (Type II). These are essential steps to establish the antiviral state where response to Interferon in chronic hepatitis C depends on the IFN-Receptor expression [11]. In the present study, the expression of IFNαmRNA together with IFNα-Rc typeI mRNA was examined in patients with HCV associated chronic liver disease (CLD) using liver biopsy specimens to investigate whether differences in expression of IFNα& INFα-Rc may be associated with the biochemical, virological and histological progress of HCV-associated CLD. Materials and Methods Patients Thirty patients with HCV associated CLD (7 patients had hepatocellular carcinoma [HCC]) participated in the present study. They comprised 12 females and 18 males aged from 29-61 years (mean±SD 45.7±8.6). All patients were followed up at KASR ELAINI Hospital Cairo University during the years 2001-2004. Patients were assessed prior to treatment by complete liver function tests, abdominal U/S, hepatitis markers and AFP on the Axsym (Abbott Laboratories USA). ANA and antibilharzial antibodies were done to exclude other complications. Finally serum HCV-RNA was extracted and analysed by the nested RT-PCR. HCV genotyping was done to confirm the diagnosis of HCV infection [12]. Liver biopsy was performed in all cases with a Trucut Biopsy Needle to decide the indication of IFNα therapy [13]. Liver biopsy specimens were divided into two parts immediately after biopsy. Half of the specimen was immersed in formalin for fixation and histological examination. The other half was immersed in HANK’s solution for RNA extraction and IFN assessment. Informed consent was obtained from all patients and their relatives prior to biopsy. Selection of patients for therapyPatients were recommended for INFα therapy when they had their liver enzymes elevated at least 1.5 times the upper limit of normal for six months, positive HCV-RNA and liver histology with at least moderate degree of necroinflammatory changes [2]. Twenty-three out of the 30 patients who were suffering from HCV only without HCC received Interferon therapy and ribavarin while the other seven patients received special therapy for HCC including IFN. Therapy protocolThe patients were treated with Regular Interferon (either Interferon Alpha 2a (Roferon-Roche, Switzerland) or Interferon Alpha 2b (Interon- Scherring, USA) and Ribavarin. An injection of 3 million units was administered 3 times per week for 24 weeks (6 months). Ribavarin was administered according to body weight (10.5 mg/kg/day) with the average dose ranging from 800 to 1000 mg/day [2]. Follow-up protocolThe twenty-three patients who were HCV positive without HCC were followed up for interferon response. Response to interferon therapy was assessed after six months of therapy initiation. Biochemical and virological response to IFN were assessed at the end of the treatment period (primary response), at week 24, and at the end of the follow up period, week 48. Biochemical response was defined as serum ALT concentrations within normal ranges and a virological response as the absence of serum HCV RNA by RT-PCR. Serum HCV RNA was confirmed by real time PCR [7,14] Nested RT-PCRRNA extraction and reverse transcription Total RNA was extracted from the serum of patients prior to treatment by acid guanidium phenolchloroform (AGPC) method. Reverse transcription was performed with 0.5 µL of 15 U/µL AMV reverse transcriptase (Amersham, Braunschweig, Germany), 4 µL RT buffer (250 mmol/L Tris-HCl [pH 8.3], 40 mmol/L MgCl2, 250 mmol/L NaCl, 5 mmol/L dithiothreitol), 4 µL of 1 mmol/L dNTPs, 0.2 µL RNase inhibitor, 1 µL of 10 µmol/L outer antisense primer, and 2.5 µL of the extracted RNA in a total volume of 20 µL at 42°C for 1 hour. Oligonucleotide primersNested RT-PCR was performed with the following primers corresponding to the highly conserved genomic sequence of the 5´-noncoding region (NCR) of HCV, 5´-CTGTGAGGAACTACTGTCTT-3´ (position 4564, outer sense12), 5´-AACACTACTCGGCTAGCAGT-3´ (position 246-265, outer antisense), 5´-TTCACGCAGAAAGCGTCTAG-3´ (position 63-82, inner sense12), 5´-GTTGATCCAAGAAAGGACCC-3´ (position 188-207, inner antisense). The resulting length of amplification products was 206 bp and 115 bp, respectively [15]. Nested PCRNested PCR was performed with 0.2 µL of 5 U/µL Taq DNA-polymerase (Boehringer Mannheim, Mannheim, Germany) in the presence of 5 µL of 1 mmol/L dNTPs, 5 µL PCR buffer (100 mmol/L Tris-HCl, 15 mmol/L MgCl2, 500 mmol/L KCl [pH 8.3]), 0.5 µL of each sense and antisense primer (10 µmol/L), and 5 µL of cDNA in a total volume of 50 µL. Five microliters of product of the first PCR diluted 1:100 was added for the second PCR. The number of cycles was 35 for each PCR, with an annealing temperature of 56°C and 60°C, respectively. Nine microliters of PCR product was run on a 2% agarose gel containing ethidium bromide [15]. HCV genotypingHCV genotyping was carried out with a second generation reverse hybridisation, line probe assay (Inno-LiPA HCV II; Innogenetics, Ghent, Belgium) according to the manufacturer's instructions with the amplified product of the nested PCR [11 ,12]. Histological studiesBiopsy specimens were fixed in 4% neutral buffered formaldehyde and embedded in paraffin. Biopsy specimens were stained with haematoxylin and eosin. Two other stainings (eosin Sirius red, Masson’s trichrome) were used for fibrosis staging. Biopsy specimens obtained were assessed for fibrosis (score 0–6) and histological activity index (HAI score 0–18) according to the scoring systems of Desmet et al and Ishak et al respectively [16,17]. A diagnosis of recurrent hepatitis was based on the presence of portal, periportal, and lobular inflammation, with lobular acidophilic bodies and/or lobular hepatocytolysis, all in the absence of endothelitis. RNA extraction and preparation of c-DNA from liver biopsySmall parts of each biopsy specimen were immediately frozen in liquid nitrogen for disruption and homogenization. Disruption was performed using a mortar and pestle and ground into a fine powder. The liquid nitrogen was allowed to evaporate but the sample was not allowed to thaw. Homogenization was necessary to reduce the viscosity of the cell lysates produced by the disruption by adding RLT Buffer. The lysate was pipetted into the QIAshredder spin column and total RNA was extracted using Quiagen RNA Extraction Kit (Quiagen Catalogue # 52304, USA) from tissue biopsies according to the manufacturer's guide. 10 ul of total RNA were transcribed to c-DNA using random hexamers primers for RT-PCR. The procedure of RT was the same as described before [17, 18]. Determination of IFNα and IFNα-Receptor gene expressionComplementary DNA (c-DNA) was used as a template for the PCR. The sequence of the primers were; IFN-α Sense: 5’ ACC TCC TGC ATC ATA CAG GC 3’, All primers were obtained from Prof Dr. Nader Abraham (director of gene therapy, Pharmacology department New York Medical College, Valhalla NY. 10509). Optimal PCR conditions were as follows; Denaturation Step: 95°C for 5 minutes (1 cycle), Amplification Step: 95°C for 1 minute, 55°C for 1 minute, 72°C for 2 minutes, this was repeated for 40 cycles, Final Extension: 72°C for 15 minutes. For each sample, individual detection of INFαmRNA and INFα-Rc mRNA was performed separately using specific primers for each of them and the same PCR conditions were followed for both. The amplified products were loaded with a loading buffer (bromophenol blue) run on 2% agarose gel. A visualized DNA band at the length 303bp was considered positive for IFNalpha and at 765bp was considered positive for IFN-Rc and at 838bp for β-actin [17, 18]. The size of the amplified product was read by the aid of a DNA marker. HCV by real time PCRAt the end of the 24 weeks of treatment and after 6 months, HCV RNA was checked in the serum of the 23 patients using Real time PCR.The majority of samples were extracted with the Roche MagNA Pure LC instrument with the MagNA Pure LC total nucleic acid isolation kit, according to the manufacturer’s instructions. HCV assay. Twenty microliters of RNA was added to 30µl of master mix for the HCV amplification and detection reaction. The Mn concentration was 3 mM. Each of the three 5' primers was at a final concentration of 360 nM, and the probes were each at 80 nM. A mixture of four different primers and two probes were used to amplify a region of the 5'untranslated region (5'UTR) of HCV. The sequence of the primers were GCGACACTCCACCATAGATCACT3, CGACACTCCACCATGAATCACT3 and CACTCCGCCATGAAYCACT (where Y is C or T). The 3' primer was CACTCGCAAGCACCCTATCA. The probes were 6-carboxyfluorescein– AGGCCTTTCGCGACCCAACACTACTC– tetramethyl carboxyrhodamine (TAMRA) and 6carboxyfluorescein– AGGCCTTTCGCAACCCAACGCTACT– tetramethyl carboxyrhodamine.[19]17 The amplification reaction was carried out in an ABI 7700 instrument with the following cycles: 50°C for 2 min, 60°C for 30 min, 95°C for 2 min, then repeat cycling of 95°C for 15 s and then 60°C for 1 min for a total of 45 cycles. Analysis was performed with the ABI SDS software and an imported ready-made standard curve was used for quantification of the samples. At the end of each run, a DNA melting step was performed, and the fusion curve was recorded to control for the homogeneity and quality of amplified DNA [11]. Statistical analysisIndividual data was summarized and presented in the form of range, mean and standard deviation as descriptive statistics. Statistical analysis was performed using the statistical software program SPSS (version 10). Two tests were performed. Chi Square test for statistical significance for determinations of associations between rows and columns was performed and Mann Whitney Nonparametric test was performed to compare means. P-value of less than 0.05 was considered significant. Results Clinical and laboratory data of patients before treatment All patients had elevated liver functions of at least 1.5 fold the upper limit of the normal, elevated AFP levels and were positive for the anti-HCV antibody. No cases showed markers for the HBV including, HBsAg, HBeAg/Ab, HbcAb nor antinuclear antibodies. Antibilharzial antibodies were below the significant limit (1/160) in all patients. Serum HCV RNA was positive in all patients. Seven patients had hepatic focal lesions and all revealed to be malignant i.e. they had HCC on top. HCC patients had a statistically significant higher mean age together with higher total and direct bilirubin and AFP levels (P-values <0.001 in all), however no statistical differences were observed regarding the rest of the liver enzymes nor the gender. HCC patients were not followed up after IFN therapy as they had a different therapeutic protocol. All patients had HCV genotype 4 however the subtypes were undetermined by the reverse hybridization, line probe assay and needed to be sequenced for determination. IFN-α and IFN-α Receptor mRNA expression in the liverAll the patients showed IFN-α gene expression except one patient who had the highest degree of fibrosis (fibrosis grade 5) and HAI Index of 9. IFNα Receptor mRNA was expressed in 30% (9/30) (Figure 4). Non of the patients with HCC had IFNα-Rc expression and the difference was statistically significant P=0.047. (Table 1). Patients with IFN-α Receptor mRNA expression had a younger mean age (P=0.01) compared to those who had no expression, while there was no other significant differences regarding gender and biochemical tests. Relationship between histological activity and IFNα-Rc mRNA Necroinflammatory activity, represented by the sum of the histological activity index (HAI) scores and the degree of fibrosis was inversely associated with the expression of IFN Alpha Receptor m-RNA (P= 0.0034 and 0.007 respectively) Fig 5&6. The higher the score, the higher the degree of inflammation and fibrosis. Relationship between IFNα-Rc mRNA expression and response to IFN therapy HCV patients without HCC were further divided according to the response of therapy. Nine patients responded while14 patients were considered as non responders as HCV RNA remained positive at the end of the 24 weeks of treatment. A significant association was found between the response to therapy and age (P= 0.004), degree of fibrosis (P=0.005) and the HAI score (P=0.001) Fig 7&8. However no association was found between the response and gender nor liver enzymes. The incidence of IFN Alpha Receptor mRNA expression was significantly higher in responders than in non-responders. Table 2 (P=0.002) HCV-RNA and IFNα-Rc m RNA expression All responders showed a negative HCV RNA result by the real time PCR, while non-respoders showed a mean 164 x 103 IU/ml ± 92 x 103 IU/ml. There was no correlation between the amount of HCV RNA after treatment in the non-responders and the expression of IFNα-Rc m-RNA. Discussion Since IFN therapy is expensive and may cause serious adverse effects, it would be clinically useful to predict the efficacy of IFN-α therapy in patients with HCV infection[20]. Despite recent treatment advances, the majority of patients with chronic HCV fail to respond to antiviral therapy. Although the genetic basis for this resistance is not clear, several factors are predictive to the response to interferon therapy. These include low amounts of HCV RNA and weaker activity of hepatitis, both predictive of favorable response to interferon. Other factors include the state of the pathology of the liver as regards inflammation, fibrosis and cirrhosis and viral genotype. There is a theory that states that deficient expression of IFN-Receptor may decrease the uptake of IFN, which results in active viral replication [21]. The current study aimed to investigate the expression IFN-α and IFN-α Receptor genes in liver biopsies from patients with HCV and HCC. Correlation of their expression with the clinical, histopathological progress of the disease and the effectiveness of IFN therapy in HCV patients after a period of 6 months follow-up was done. Comparison between HCV patients & HCC patients regarding the clinical & laboratory findings didn’t reveal any significant differences except for Bilirubin and AFP levels indicating an obstructive element in patients which is higher with HCC [22]. Interferon Alpha mRNA expression was detected in 29 out of 30 patients (96.7%), only one patient was negative for IFN Alpha gene who had marked liver fibrosis & high histological activity index (HAI>12). Since an anti-viral state is established not by IFNα molecule itself but by proteins induced by IFNα, the binding of IFNα to specific receptors and intracellular signal transduction after IFNαReceptor binding are essential steps to establish the anti-viral state. Thus, the response to Interferon in chronic hepatitis C depends on the INFα-Rc in the liver. [5,23] Interferon Alpha Receptor (IFNα-Rc) mRNA expression was found in 30% (9/30) of our patients. Findings confirmed that patients who expressed IFNα-Rc were characterized by younger age group, better histopathological findings (lower degree of fibrosis) and lower HAI score. However no statistical significant difference was observed regarding gender, other clinical and laboratory findings. The difference in age may be due to the 7 patients suffering from HCC on top of HCV, for whom the mean ages (56.6 ± 4) was higher than the group suffering from HCV alone (42.1 ± 6.6) since HCC is a complication of HCV. Moreover, patients who were suffering from HCC on top of HCV were all in the receptor-negative group [17, 22]. Frequency of receptor expression was higher among the HCV patients and none of the patients who developed HCC had receptor expression. HCV related HCC shows stepwise regression from chronic hepatitis with progressive stages of fibrosis to cirrhosis and eventually clinically apparent HCC. Since all patients who developed HCC in the present study also had marked liver cirrhosis thus were showing an advanced histopathological picture and distortion in the liver architecture. Other studies had also stated that the amount of receptor expression is inversely proportionate to the pathological status of the liver [1,24] thus we can explain that the absence of receptor expression in HCC positive cases stems from this logic. One possibility for the decrease in the gene expression with histological progress may be that the gene expression of IFNα-Rc itself becomes suppressed during histological progress [25]. Another theory also supports the fact that continuous inflammation in the liver may cause some changes in protein synthesis [11]. Thus down regulation of IFNα gene expression will decrease IFNα protein production and hence IFNα-Rc binding, which will finally down regulates IFNα-Rc gene expression [10]. This can be attributed to the theory of suggesting that the lower expression of IFNα-Rc mRNA may be partially responsible for the poor response to IFNα in liver cirrhosis [4,5,10,11,23,24]. Of our 23 HCV patients, 9 showed sustained virological response to IFNα. Responders to therapy were seen to show significantly lower mean age, better histopathological states (lower grades of fibrosis and better grade of HAI) and higher incidence of expression of IFNα-Rc mRNA and the differences were statistically significant. Several variables have been established as being associated with a greater likelihood of sustained virological response to interferon therapy [7] Morita et al., found that the presence of IFNαR1 or IFNαR2 mRNA predicted complete response to interferon treatment, with a positive predictive value of 100% [26]. Later in 1999 [27] they found that IFNα-Rc mRNA expression and the absence of genotype 1b were significant predictors of sustained biochemical and virological effectiveness of IFNα therapy. They added also that the absence of HCV genotype 1b, low titer of HCV RNA and expression of IFNα-Rc mRNA were significantly correlated with the sustained virological and biochemical response to interferon treatment. This may suggest that a poor response to IFN may result from deficient expression of the receptor. It has been explained that deficient expression of IFNα-Rc may reduce the uptake of IFNα, which results in increased viral replication and more severe hepatitis activity which leads to inflammation, increase IFN production and fibrosis, thus the resistance of response to therapy [5,25,28]. Conversely, 2 of our responders were IFNα-Rc negative and 2 of the non-responders expressed IFNα-Rc m-RNA. This can be explained by 1) a difference in intracellular signal transduction after receptor binding, 2) the presence of IFN sensitivity determining region (ISDR) in the different HCV patients because some IFN resistant cells may express functional receptors, 3) the binding affinity of the IFNα-Rc may be changed in non-responders despite the presence of IFNα-Rc molecules [8]. Further analysis of the amount of HCV RNA by real time PCR in the non-responders revealed that it had no association with the pretreatment expression of IFNα-Rc. Morita et al stated that a low titer of HCV RNA was not an independent predictor of IFN efficacy [27]. Another study found that IFNα-Rc m-RNA expression in 20 liver patients was significantly higher than 6 normal patients but the level did not correlate with the amounts of serum HCV RNA [15]. Although Fukada et al found that there was an inverse correlation between the amount of HCV RNA and the amount of IFNα-Rc m-RNA in both responders and non-responders [18], Fujiwara et al [23] stated that HCV-RNA level is independently associated with a sustained virologic response. This may be due to the lack of studies done on the HCV 4 genotypes and subtypes regarding, its correlation with IFNα-Rc m-RNA expression. Further study using a large number of patients is clearly necessary to explain the difference [29]. HCV RNA dependant RA polymerase (RdRp), like other viral RNA polymerases, has a high error rate, with misincorporation frequencies averaging about 10-4 to 10-5 per base site, due to the absence of a proofreading mechanism. As a result, mutations accumulate in newly generated HCV genomes. Most mutant viral particles are replication deficient, but some propagate efficiently. The fittest infectious particles are selected continuously on the basis of their replication capacities and environmental selective pressures (mainly the host immune response). This explains why each infected individual harbors a pool of genetically distinct but closely related HCV variants referred to collectively as a quasispecies [8,30]. This may explain the lack of determination of the subtypes in our patients which need sequencing to differentiate between subtypes of genotype [4 [2]. ConclusionWe can conclude that Interferon Alpha Receptor Expression decreases with the histological progress of the disease inspite of the presence of IFNαm-RNA in most of our patients suggesting that lower expression of the Interferon Alpha Receptor mRNA may be partially responsible for the unfavorable response to interferon for patients with an unfavorable histopathological picture and may be a predictor of interferon response in chronic hepatitis C. Also, there was no association between the IFNα-Rc m-RNA expression and serum ALT level, and amount of serum HCV RNA or HCV genotype. It’s recommended to Quantitate the amount of interferon alpha receptor mRNA expression in order to further analyze if the quantity is related to the outcome. However, investigation of the amount of IFN-Rc mRNA in the liver is not appropriate for routine examination before IFN therapy in all patients, thus investigating IFN-Rc associated molecules or its expression in peripheral blood mononuclear cells could be performed aiming to avoid the invasive biopsy procedure if a correlation could be detected. Finally studies involving the relationships between interferon alpha receptor mRNA expression and genotype and subtype in Egypt might also prove useful. References
Copyright 2007 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh07012f2.jpg] [jh07012f5.jpg] [jh07012f8.jpg] [jh07012f6.jpg] [jh07012f1.jpg] [jh07012f4.jpg] [jh07012f7.jpg] [jh07012t2.jpg] [jh07012f3.jpg] [jh07012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}