 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
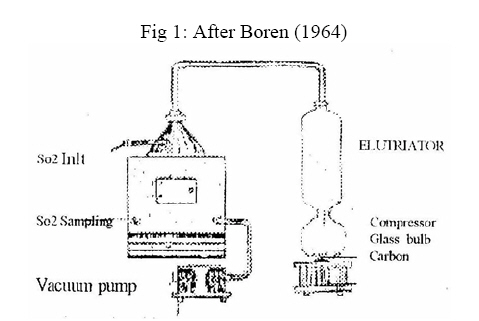
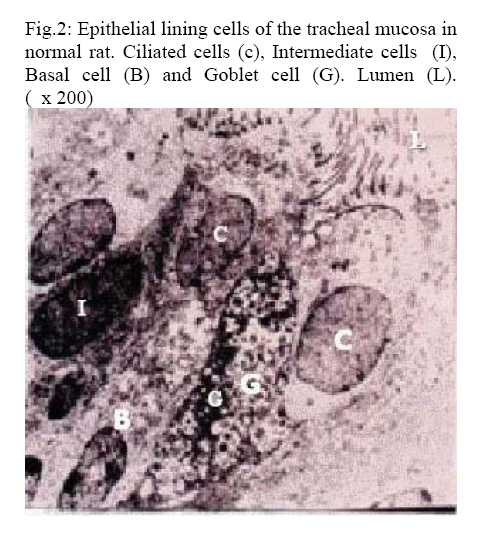
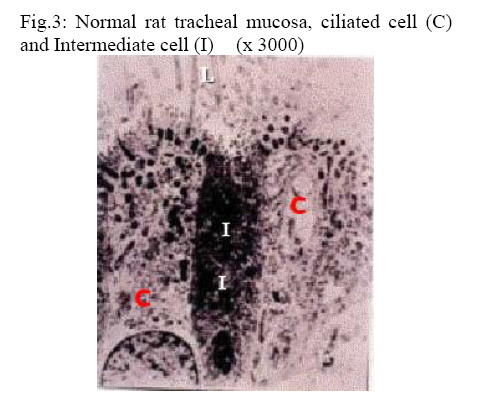
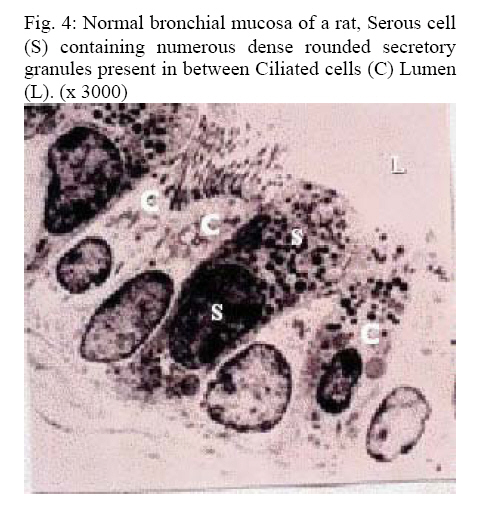
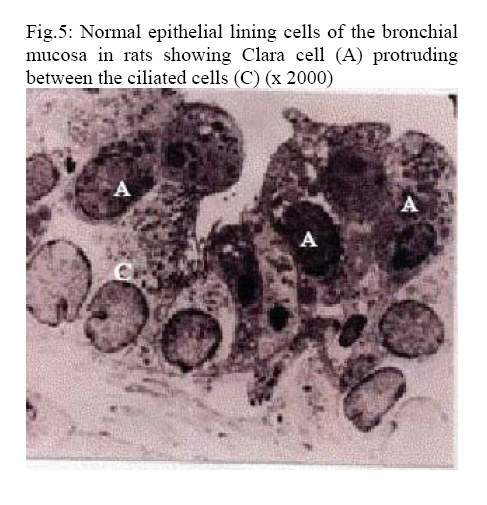
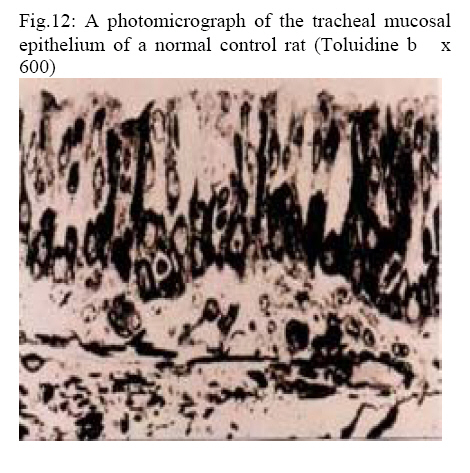
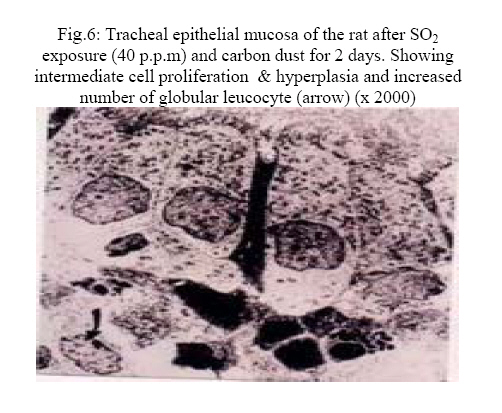
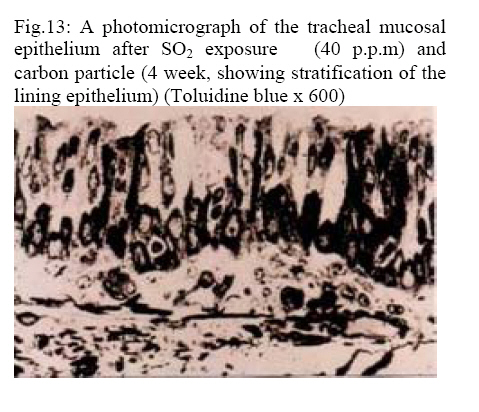
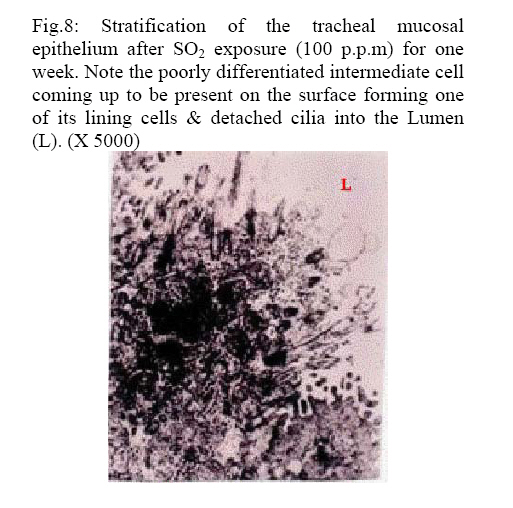
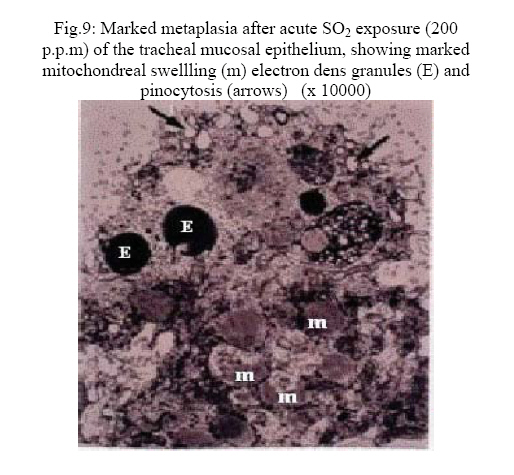
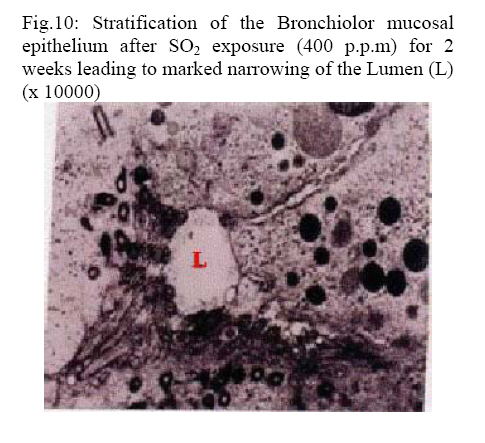
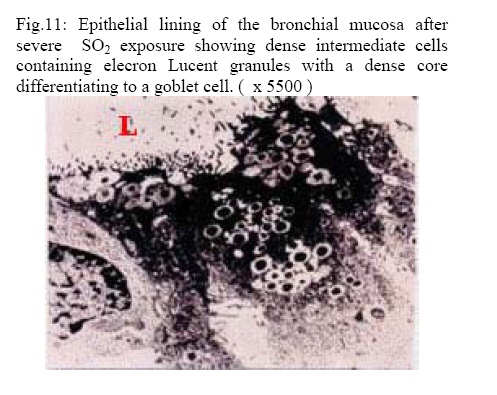
African Journal of Health Sciences, Vol. 14, No. 3-4, Jul-Dec, 2007, pp. 129-136 Ultrastructural study of the effect of air pollution by SO2on the respiratory air-ways Ibrahim L. Abdalla Faculty of Medicine, Cairo University, Egypt Code Number: jh07019 SUMMARY Sulfur dioxide (SO2 ) has been associated with excessive mortality during air pollution disasters such as that which occurred in Meuse Valley, Belgium in 1930, Donora Pennsylvania, in 1948and London in 1952. The SO2 particulate complex results chiefly from the burning of fossil fuels. Exposure can cause irritant and toxic effects on the human airways and result in broncho- constriction. It also can aggravate existing pulmonary or cardiac problems. A positive interaction between particles and SO2 to produce morphologic changes in airways has been suggested by smog incidents, but has not been evaluated by experiments. So, this study was done to answer the following questions: (1) What morphologic changes are produced by repeated injury to airway epithelial cells by SO2? (2) What is the time course of these morphologic features? (3) Can a model of acute bronchitis be created which is not due to infection? Ultrastructural changes occurring in the epithelial cells lining the airways of the experimental rats were studied. A sequence of epithelial changes was seen with exposure to 100, 200 or 400 p.p.m. for up to 4 weeks. For example: loss of cilia, vacuolation, pyknosis, goblet cell hyperplasia and the development of stratified squamous epithelium after 2 to 7 days at 200 p.p.m Higher doses (400 p.p.m.) produced squamous cell metaplasia after 2 weeks. Exposure to 40 p.p.m. SO2 alone for 4 hours per day for 6 weeks produced no changes, but 24 hours after a 4 hours exposure to 40 p.p.m. SO2 plus 0.74 gm of carbon dust per cu.m. of air, neutrophils were recruited into airway epithelium. It is suggested that this synergistic effect is due to the carbon particles adsorbing SO2, which leaches off slowly, perhaps within macrophages, to recruit Leucocytes in airways. Introduction Sulfur dioxide (SO2) has been associated with excessive mortality during air pollution disaster such as that which occurred in Meuse Valley, Belgium in 1930, Donora Pennsylvania in 1948and London in 1952 [1, 2, 3]. The morphologic changes in the lung produced by Sulfur dioxide (SO2) have been studied in various animals [4, 5, 6, 7]. Sulfur dioxide SO2 and sulfuric acid are also common in industry.’ In 1974 the National Institute for Occupational Safety and Health (NIOSH) estimated that 500.000 workers could be exposed to SO2 [8]. It may be encountered in a variety of industries in the production of paper, in refrigeration plants, fruit processing, manufacturing of sodium sulfite and petroleum refining. Although outdoor air contamination by SO2 or acidic aerosols has been the focus of concern, Kerosene Space heaters are now recognized as an important indoor source of sulfur dioxide, sulfates and acidic aerosols [9, 10]. Indoor levels may exceed maximum outdoor levels of SO2 by 10 times or more. Since most persons spend the majority of time indoors, for many pollutants the indoor environment is a major determinant for total exposure. Experimental studies of human subjects exposed to SO2 and acidic aerosols under carefully controlled conditions can demonstrate immediate responses to various levels of these pollutants. The most striking effect of acute exposure to SO2at concentrations of 1.00 p.p.m. or lesswas the induction of bronchoconstriction in asthmatic patientafter only 5 minutes exposure. In contrast, inhalation of concentration of SO2in excess of 5 p.p.m. was shown to cause decrements in airway function in normal subjects [11, 12, 13, 14]. The SO2particulate complex results chiefly from the burning of fossil fuels. Exposure can cause irritant and toxic effects on the human airways and result in bronchoconstriction. It also can aggravate existing pulmonary or cardiac problems. A positive interaction between particles and SO2 to produce morphologic changes in airways has been suggested by smog incidents, but has not been evaluated by various experiments [15-21]. Concerning the dangerous effects of sulfur dioxide SO2 and other air pollutants on the vital organs e.g. the lungs and heart Routledge et al. [22] confirmed the work of Fusco et al [23], Matooane and Diab [24], Wichmann [25] and Blauchard and Hidy [26], they reported that gaseous air pollutants were important determinant of acute hospitalization for respiratory conditions and asthma they added that exposure to urban air particulates alters the macrophage mediated inflammatory response to respiratory vital infection. Triche et al. [14] concluded that secondary heating appliances are important sources of air pollution, including paticulate matter, nitrogen dioxide (NO2) and sulfur dioxide (SO2), and they reported emissions from fireplaces, gas space heaters and kerosene heaters might contribute to respiratory symptoms e.g. chest tightness, wheezing, sore throat and cough So, this study was done to answer the following questions: (1) What morphologic changes are produced by repeated injury to airway epithelial cells by SO2?. (2) What is the time course of these morphologic features? (3) Can a model of acute bronchitis be created which is not due to infection? Material and Methods 25 male albino rats of the Sprague-Dawley strain weighing 190 – 215 gm. were used in this study. The animals were classified into 2 groups: Group I: Including 5 animals used as controls and exposed to filtered room air. Group II: Including 20 rats, these were subdivided into 4 groups (Experiments): Which exposed to different concentration of SO2. 100, 200, 400 p.p.m. (part per million) and 40 p.p.m. (alone and with carbon dust). The food and water were removed during exposure hours (also from control animals), but otherwise, food and water were provided ad libitum. Exposures were carried out in cuboidal plexiglass chambers of approximately 1.5 cu. ft volume (Fig. 1) designed by Boren [27] and based on principles described by Silver [28]. Room air was delivered into the chamber through circular louvers from a filter per minute by removing air from the animal hold portion by a perforated stainless steel floor. It held a drawer for removing droppings and urine. Sulfur dioxide from a cylinder was led through a Teflon manifold into the chambers so that three exposure chambers could be operated simultaneously and the concentration in each chamber could be varied independently of the other (100, 200 and 400 p.p.m.). The SO2 flow into each chamber was measured with ”Gilmont Flowmeters (personal Sampler Apparatus). Exposure was for 5 hours per day. 5 days per week for the previous three concentrations for up to 4 weeks. A cute exposure experiments of 5 hours single exposure were carried out on the 4thgroup of rats. Exposure to 40 p.p.m. SO2 was combined with exposure to carbon dust. 0.74 gm per cu.m. in one 4-hour experiment. The dust was generated in a large glass bulb with a magnetic stirrer, and compressed air flow (Fig. 1). The dust ascended through an 80 cm tall vertical elutriator to eliminate the larger particles and entered the chamber from the top. SO2 entered through an injector in the center of the conical top. Chamber gas was removed through the perforated floor. The animals dying spontaneously during exposure were autopsied immediately. Others were anesthetized with 12 mg. of sodium pentobarbital (Nembutal) intra-peritoneally at the time of sacrifice. With sterile methods. The trachea was exposed and ligated just below the larynx. The chest was then opened and the trachea and lungs were exposed by dissection and injected in situ via the trachea with 3% buffered glutaraldehyde (0.1 M. sodium cacodylate at pH 7.4) then they were removed, fixed in this solution for 18 to 24 hours. Sections for electron microscopy were selected from the trachea, bronchi and bronchioles and cut into 1 to 2 mm. Cubes. These were post fixed in 1 % osmium tetroxide, dehydrated in increasing concentrations of ethanol 35 to 100 per cent folloved propylene oxide, and embedded in epoxy resin (Epon). One micron thick sections were cut on LKB ultramicrotome, and stained for 4 – 5 minutes at 60 C with freshly prepared and filtered toluidine blue and then were examined .by light microscopy. Ultra-thin sections were cut after trimming the blocks, picked up on copper grids, stained with 4% uranyl acetate and lead citrate and examined in a Zeiss Ell 9 electron microscope. Results Control rats exposed to filtered air showed normal tracheobronchial epithelium and lamina propria (Fig. 2,3,4,5 and 12) while the rats exposed to 40, 100, 200 and 400 p.p.m. Sulfur dioxide SO2 produced epithelial damage in large airways in all groups after 1 week (20 hours) of exposure. The changes became more severe, extensive, and further peripherally with higher concentrations of Sulfar dioxide SO2 and longer exposures. Exposure to 40 p.p.m. of Sulfur dioxide SO2 for 1 to 4 weeks produced some loss of cilia and vacuolation of ciliated cells in the trachea which became extensive during the last weeks of the experiments. Fewer changes were seen in the major bronchi but no changes were found in the bronchioles. Exposure to 40 p.p.m. SO2 alone for 4 hours/day for 6 weeks produced no leucocytes recruitment after 2 days from the beginning of exposure. However, when exposure was to Sulfur dioxide SO240 p.p.m. and carbon dust 0.74 gm. Per cu.m. combined, numerous polymorph nuclear leucocytes were seen within bronchial walls and in the lumen, one day after beginning exposure (Fig. 6 & 13). Exposure to 100 p.p.m. of SO2 produced in the trachea more extensive loss of cilia, degeneration of ciliated cells and areas of basal cell hyperplasia. There were less extensive changes in the bronchi, but all bronchioles appeared normal. (Fig. 8) Five days of exposure for 5 hours per day to 200 p.p.m. showed squamous metaplasia and large areas of basal cell hyperplasia. Most cells were vacuolated, showed dense staining and pyknosis and disappearance of cilia. Bronchi showed loss of cilia and cellular degeneration but neither basal cell hyperplasia nor squamous metaplaisa. Bronchioles appeared normal. Polymorph nuclear leucocytes were recruited into the epithelium of the ’tracheobronchial tree. The ciliated and goblet cells were much taller and wider than controls, and intercellular spaces were wide and vacuolated.The endoplasmic reticulum was extensively dilated and vacuolated and mitochondria were swollen and vacuolated. (Fig. 9) Rats exposed to 400 p.p.m. SO2: The rats became restless and severely dyspneic immediately after the beginning of exposure to SO2. Three rats died at the end of first 5 hours exposure. After the first week of exposure, the remaining 2 rats seemed to tolerate the gas better and stayed inactive during the exposure, they died after 14 days of the experiment. The tracheo- bronchial trees of these group were removed after death and were studied. In comparison with the control (normal non-exposed) rats. Tracheas showed epithelial degeneration, loss of cilia, infiltration of leucocytes, and desquamation. In 2 rats, squamous metaplasia was found. Effects were diminished toward distal airways. Bronchi and some bronchioles showed the vacuolar degeneration and areas of necrosis similar but less extensive than that of the tracheas (Fig. 10 & 11). Discussion The main primary pollutants released into the atmosphere are sulfur dioxide (SO2), nitrogen monoxide (NO) and dioxide (NO,), particulate dust and in a less important part carbon monoxide (CO). Sulfur dioxide is soluble in water and therefore absorbed on a wet mucous membrane. Thus 90 to 95 per cent of SO2in the 100 to 130 p.p.m. concentration range was absorbed on the nasal mucosa [29, 30, 31]. Such absorption undoubtedly continues down the respiratory tree so that exposure of epithelial cells to the gas becomes less and less. This would explain why the greatest mucosal changes were always seen in the trachea and larger bronchi but the bronchioles were invariably spared, even in the animals dying fromSO2 exposure. The histological changes and the pathological, toxic, and degenerative alterations in the airways epithelia and the increase in the number of secretory granules and vesicles, which were observed in this present experiments coinced with the studies of Goldring et al.; Lawther et al. ; Llacuna et al. and Min et al. [5, 18, 32, 33]. In this study, leucocyte recruitment resembling purulent bronchitis was seen after a high dosage of SO2 (200 p.p.rn. and after simultaneous exposure to a lower dosage ofSO2 (40 p.p.m.) and carbon dust. Maximal recruitment was seen 24 hours after the beginning of exposure. This delay in response to SO2and carbon suggest that it may set up a chain of events leading to leucocytes recruitment carbon particles potentate effects of irritant gases on the peripheral airways as noted by Boren [27]. It is suggested that this synergistic effect is due to the carbon particles adsorbing SO2, which leaches off slowly, perhaps within macrophages, to recruit leucocytes in airways [19, 34, 35, 36]. Epidemiological data addressing the role of air pollutants at usual levels can only suggest that some pollutants (Sulfur dioxide SO2 suspended particulates) constituted a risk factor for respiratory infections. La Dou; Aris et al.; Atzori et al. and Barnes [35] reported that when the level of SO2 were exceptionally high, it was possible that asthmatic patients might have increased symptoms after exertion. Since this irritant gas acts as a trigger to broncho-constriction [13, 15, 31, 35]. Steinman et al. studied the Sulfur dioxide sensitivity in South African asthmatic children and pointed out that there were many food stuffs that were preserved with SO2 and other sulfites e.g. apple juice which might precipitate asthmatic attacks [17]. Hajat et al., Aekplakorn et al. and Pino et al. studied the effects of fine particulate matter and wheezing illnesses in children and reported stronger effects for Sulfur dioxide (SO2), Nitrogen monoxide (NO) and Nitrogen dioxide (NO2) and concluded that air pollution in the form of fine particulates, mostly from vehicular exhaust might adversely affect infants respiratory health with potential for chronic effects later in life [20, 36, 37]. Animal experiments demonstrated that air pollutants decreased the efficacy of lung defense mechanisms, and increase the sensitivity to respiratory infections. Nevertheless, because of the difference in sensitivity between animal species and between exposure conditions, these effects were difficult to extrapolate to humans. Moreover, it is obvious that direct exposure studies of sensitivity of humans to respiratory infections were rare for ethical reasons. Conclusion The present study and findings think that high concentration of air pollutants are very likely to increase susceptibility to respiratory infections in humans and precipitate asthmatic attacks. It can be suggested that, since sulfite sensitivity is common in asthmatic people, ingestion of sulfites should be avoided e.g. apple juice. Also, it was shown that the penetration of SO2 to the lungs was greater during mouth breathing than during nose breathing [32, 35]. There is increased uptake in persons exercising and/or mouth breathing during incidents of heavy pollution. Recommendation In view of the present study results, it can be recommended that:
References
© Copyright 2007 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh07019f5.jpg] [jh07019f14.jpg] [jh07019f4.jpg] [jh07019f15.jpg] [jh07019f6.jpg] [jh07019f1.jpg] [jh07019f8.jpg] [jh07019f7.jpg] [jh07019f2.jpg] [jh07019f10.jpg] [jh07019f13.jpg] [jh07019f3.jpg] [jh07019f9.jpg] [jh07019f11.jpg] [jh07019f12.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}