 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
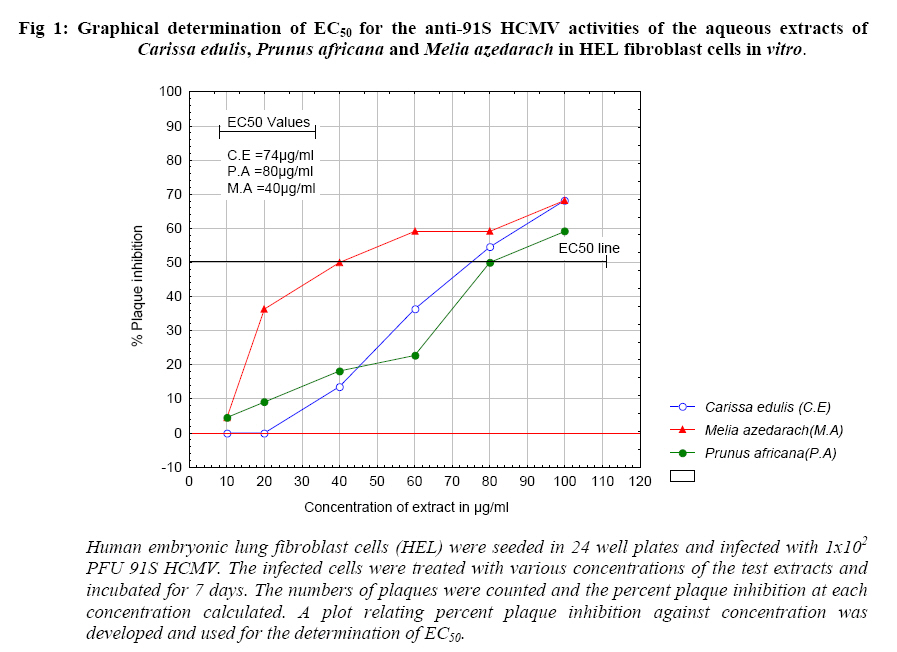
African Journal of Health Sciences, Vol. 14, No. 3-4, Jul-Dec, 2007, pp. 143-148 In vitro anti-viral activity of aqueous extracts of Kenyan Carissa edulis, Prunus africana and Melia azedarach against human cytomegalovirus Festus M. Tolo1,7*, Geoffrey M.Rukunga 1,7, Faith W. Muli 4, John Ochora 6,7, Yoshito Eizuru2,5, Charles N. Muthaura1, Cecilia W. Kimani1, Geoffrey M Mungai3 and Mawuli W.Kofi-Tsekpo1 1Kenya Medical Research Institute, Code Number: jh07021 SUMMARY The aqueous extracts of three medicinal plants, Carissa edulis (Forssk.) Vahl (Apocynaceae), Prunus africana (Hook.f.) Kalkm (Rosaceae) and Melia azedarach L. (Meliaceae) have shown significant reduction in the replication of human cytomegalovirus (HCMV) in human embryonic lung (HEL) fibroblasts cells in vitro. Using the plaque inhibition assay for the determination of anti-viral activity, the HEL fibroblast cells cultured in 24 well plates were infected with 1 x 102 PFU 91S HCMV and treated with various concentrations of the extracts. The plaques formed were counted after 7 days incubation at 370C in 5% CO2 and the percent plaques inhibited were calculated against infected untreated control. The effective concentrations inhibiting plaque formation by 50% (EC50) was found between 40 to 80 µg/ml for all the extracts. The cell cytotoxic concentrations (CC50) for each of the three extracts, by the trypan blue exclusion test, gave a safe therapeutic index. These results have demonstrated the potential anti-viral activities of the extracts of the three medicinal plants at non-cytotoxic concentrations. Introduction Human cytomegalovirus (HCMV), a b-herpesvirus in the family herpesviridae, is found universally throughout all geographic locations and socioeconomic groups [1]. The HCMV is the virus most frequently transmitted to a developing child before birth (0.2-2.2% of all live births) [2]. For most healthy persons who acquire HCMV after birth,there are few symptoms and no long-term health consequences. However, HCMV infection is one of the most challenging complications in persons with lowered immune states as experienced after hematopoietic stem cell transplantation (SCT) or solid organ transplantation (SOT) [3,4] and in persons with Acquired Immunodeficiency Syndrome (AIDS) [5]. In such instances, HCMV disease may occur as organ involvement such as pneumonitis or as an indirect effect such as an increased risk of opportunistic infections [6,7]. The most widely used drugs for prophylaxis and treatment of HCMV infections are foscarnet, cidofovir and ganciclovir. Unfortunately, these drugs have dose limiting renal and bone marrow toxicities. Also the long-term therapy with these drugs, necessary for management of infection, has been associated with development of clinically resistant strains of the virus [8, 9,10,11]. Therefore, antiviral agents would need to be developed for the treatment and suppression of HCMV disease. Natural products of plant origin are proving to be a valuable source for anti-viral agents [12,13,14]. We hereby report on extracts from three medicinal plants that grow in Kenya which have shown significant activity against HCMV in vitro. The plants are Carissa edulis (Forssk.) Vahl (Apocynaceae), Prunus africana (Hook.f.) Kalkm (Rosaceae) and Melia azedarach L. (Meliaceae). The three medicinal plants are widely used traditionally for treatment and management of various disease conditions by different communities in Kenya and their use in traditional medicine is well documented [15,16,17]. Materials and Methods Medicinal plant material collection The medicinal plants used in this study were collected with the assistance of the taxonomist, Mr. G.M. Mungai, from the East African Herbarium, Nairobi, Kenya. The plants were obtained from their natural habitats in different geographical zones of Kenya. Carissa edulis was collected from Gitoro forest, Meru District in Eastern Province. Prunus africana was colleted in Taita hills, Taita-Taveta District, Coast Province and Melia azedarach was collected in Karura Forest, Karura, Nairobi Province. Voucher specimens were on deposit at the East African Herbarium, Nairobi, Kenya. The stem and root barks were chopped into small pieces and dried at room temperature for two weeks. The dry barks were ground into fine powder using an electric mill (Christy and Norris Ltd., England) and stored in plastic containers at room temperature ready for use. A 100g of stem or root bark powder was boiled in 1000 ml distilled water for 45 min. The resulting extracts were filtered and lyophilised using a Modulyo Freeze Dryer (Edwards, England) producing a free flowing powder that was weighed and stored in airtight containers at room temperature until use. Each of the freeze dried material was treated as follows:- A 10 mg/ml stock solution was prepared by dissolving 100 mg of the freeze-dried powder in sterile double distilled water and made to the 10mls mark of a volumetric flask. The solution was centrifuged at 3,000 rpm for 15 min (Kubota centrifuge, Japan) to separate any un-dissolved matter and the supernatant collected and filtered through a 0.45 µm membrane filter. The sterile filtrate was stored at 40C and used as a stock solution within a week. For the in vitro experiments, a working solution of 1 mg/ml was aseptically prepared by diluting 100 µl stock with 900 µl (0.900 ml) Eagle’s Minimum Essential Medium (MEM) (GIBCO BRL, Scotland) supplemented with 2% Fetal Bovine Serum (FBS) (GIBCO BRL, Scotland). Viruses and cells The gancyclovir-sensitive clinical isolate of HCMV strain 91S and human embryonic lung fibroblast cells (HEL) were used in the study. The virus and cells were donated by the Kagoshima University, Kagoshima, Japan, through the Japan International Cooperation Agency (JICA). The virus was propagated in HEL cells of persurge numbers between 17 and 18. The infected cultures were sonicated on ice and centrifuged at 3,000 rpm for 15 min. The virus stock (supernatant) was stored in 35% sorbitol (Sigma) at -800C until use. The HEL cells were grown and maintained in Eagle’s Minimum Essential Medium (MEM) (GIBCO BRL, Scotland) supplemented with 10% (for cell growth) or 5% (for cell maintenance) heat inactivated fetal bovine serum (FBS) (GIBCO BRL, Scotland), kanamycin (60µg/ml), and 0.12% sodium hydrogen carbonate (NaHCO3) (Sigma). Reference drug gancyclovir Gancyclovir was used as a reference drug and was a donation from Prof. Yoshito Eizuru of the Division of Persistent and Oncogenic Viruses, Centre for Chronic Viral Diseases, Faculty of Medicine, Kagoshima University, Kagoshima, Japan and who was also a JICA visiting scientist at the Kenya Medical Research Institute (KEMRI). Plaque reduction assay The freeze-dried aqueous extracts of the medicinal plant materials were examined for extent of reduction of plaque formation on infected HEL cells in vitro. Briefly, HEL cells were cultured in MEM supplemented with 10% FBS to a confluent monolayer in 24-well plates at 37 0C in a 5% CO2 incubator (Hirasawa Works, Japan). The culture medium was aspirated off aseptically and the cells infected with 100 plaque forming units (PFU) of 91S HCMV. The virus was left to adsorb for 1 hr at room temperature on a tray shaker. The cells were then overlaid with maintenance medium containing 2.25% methylcellulose (MC), 5% FBS, 0.24% NaHCO3 and various concentrations of freeze dried extracts (10 ~ 100 µg/ml) or gancyclovir at 5 µg/ml. Each concentration was done in triplicate. The plate was incubated at 37 0C under 5% CO2 for 7 days. At the end of the incubation period, the cells were fixed by adding 0.5ml of 5% formalin (Sigma) solution into each well and left to stand for 1 hr. The media in each well was decanted and the cells stained with 0.03% methylene blue solution (Wako Pure Chemical Industries Ltd., Japan). The plaques, appearing as transparent dots were counted under a dissecting microscope with the aid of an electronic marker pen. The percent plaque inhibition was calculated and the effective concentrations for 50% plaque inhibition (EC50) were determined from a plot relating percent plaque inhibition against extract concentrations [18]. Cell cytotoxicity assay The cell cytotoxicity of the extracts was evaluated in vitro by the trypan blue exclusion test as described elsewhere [11]. Briefly, 6x104 HEL cells were seeded in 24-well plates in MEM supplemented with 10% FBS and incubated at 370C in 5% CO2 to a confluent monolayer. The culture medium was replaced by fresh medium containing various concentrations of the freeze-dried extracts and the cells further incubated for 1 day. Each extract concentration was done in triplicate. The cells were treated with trypsin and the number of viable cells determined by the trypan blue exclusion test. The concentration of extract reducing cell viability by 50% (CC50) was determined from a curve relating percent plaque inhibition against concentration. Data management Plaque inhibition assay In the plaque inhibition assay, the number of plaques in the infected untreated cells (control) and the number of plaques in the infected treated cells (test drug) was used for the calculation of the percent plaque inhibition using the formula below:
The percent plaque inhibition at each extract concentration was then used for the graphical determination of EC50. Cytotoxicity assays In the cell cytotoxicity determinations, the number of viable cells was used for the calculation of percent cell viability at each tested extract concentration. This was then used for the graphical determination of the cell cytotoxic concentration (CC50). Results The following results were obtained when infected and non-infected HEL cells were treated with the various concentrations of the freeze-dried plant extracts. Table 1 and Figure 1 show the results of the in vitro quantitative evaluation of anti-viral activity of the plant extracts in HEL cells infected with 91S HCMV. The following were the responses to various extract treatment as illustrated in Table 1 and Figure 1. Treatment with the Melia azedarach extract There was a rapid rise in plaque inhibition from 5% to 36% between the 10µg/ml and 20µg/ml extract concentrations (Figure 1). Thereafter plaque inhibition increased with rise in extract concentration, 50% of the plaques being inhibited at 40µg/ml (Figure 1. Table 1 shows the percent plaques inhibited at each tested extract concentration. Treatment with the Carissa edulis extract There was no plaque inhibition between 10µg/ml and 20µg/ml concentrations. However inhibition was observed at concentrations above 20µg/ml in a dose related manner. The effective concentration inhibiting 50% of the plaques (EC50) was at 74.0µg/ml (Figure 1). Table 1: The percent plaque inhibition in HEL cells infected with HCMV at 1x102 PFU/10µl and treated with extracts at various concentrations.
Human embryonic lung fibroblast cells (HEL) were seeded in 24 well plates and infected with 1x102 PFU 91S HCMV. The infected cells were treated with various concentrations of the test extracts and incubated for 7 days. The numbers of plaques were counted and the percent plaque inhibition at each concentration calculated against uninfected control Treatment with the Prunus africana extract Plaque inhibition increased steadily with increase in concentration. The EC50 was obtained at 80µg/ml (Figure 1). Cell cytotoxicity assay Table 2 presents the cell cytotoxic concentrations for 50% cell death (CC50) of the extracts in non-infected HEL cells. The EC50 values are also included in this table for comparison. The results show that the CC50 values for all the extracts were above the EC50. The Melia azedarach extract was cytotoxic at concentrations above 80µg/ml while the Carissa edulis and Prunus africana extracts were cytotoxic at concentrations above 100µg/ml. Table 2: The cell cytotoxic concentrations (CC50) and the effective concentrations for 50% plaque inhibition (EC50) for Carissa edulis, Prunus africana and Melia azedarach aqueous extracts in HEL fibroblast cells in vitro.
In the CC50 determination, the HEL fibroblast cells were seeded in 24 well plates at 6x104 cells/well and treated with various concentrations of the extracts. The trypan blue exclusion test was used for evaluation of cell viability at each tested concentration. The concentration of extract reducing cell viability by 50% (CC50) was determined from a curve relating percent cell viability to concentration. Discussion The results indicate that the HCMV strain 91S used in the study was sensitive to all the three extracts examined. However, the virus was more sensitive to the Melia azedarach extract than to the other two from Prunus africana and Carissa edulis whose activity was almost similar (the EC50 for both being very close, 80µg/ml for the Prunus africana extract and 74µg/ml for the Carissa edulis extract). In an earlier investigation where the extracts had been examined for in vitro anti-herpes simplex virus type 1 and 2 activity, a significant antiviral activity was also observed [13]. The results of this study therefore show that the extracts have an extended antiviral activity for both the alpha (a) and beta (b) members of the herpesviridae family. This is an encouraging finding and calls for the determination of the mode of antiviral action of these extracts to compare with those of known antivirals such as acyclovir and its derivatives [19,20,21]. It is important to note that the medicinal plants whose extracts were investigated for antiviral activity belong to different families yet all of them exhibited reasonable antiviral activity. This indicates the possibility of the plant extracts having substances common in nature which poses potent antiviral activity. It also explains why different medicinal plants are used for the management of one single disease condition. Conclusions At this point, the only conclusion that can be drawn of these results is that the three medicinal plant extracts have shown potential as anti-91S HCMV agents in vitro. It is necessary to investigate these activities in vivo. Since the extracts of some of the plants had shown promising activity against HSV in both the in vitro and in vivo environments (13), it is envisaged that they could also do the same to the HCMV. If this turns out to be the case, then these plants could be of high potential as sources of anti-herpesvirus agents. Natural products of plant origin have been found to contain antiviral properties worldwide [12,13,14,18]. Therefore there are possibilities of future antivirals being derived from plants or their constituents. This, in a way, puts Sub-Saharan Africa at an advantageous position due to her abundant resource in medicinal plants. It is therefore a great challenge to the scientists in the region to ensure that this available resource is tapped for the befit of our people. Acknowledgments The authors are grateful to the Japan International Cooperation Agency (JICA) for the financial and technical support in this study and to the Director, KEMRI, for authority and permission to publish these results. We also thank Mr. L. Ogutu, Ms. M. Muthoni, Ms. G. Nginya, Mr. D. Odira and Mr. N. Mwangi for their excellent technical assistance. References
© Copyright 2007 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh07021f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||


{kind=link}