 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Health Sciences, Vol. 14, No. 3-4, Jul-Dec, 2007, pp. 164-170 A study of the pharmaceutical quality of chloroquine and paracetamol products sold in a major Nigerian “market” Justina O Ofonaike¹, Ehijie FO Enato² Augustine O Okhamafe³ 1 Department of Pharmacy, Federal Medical Centre,
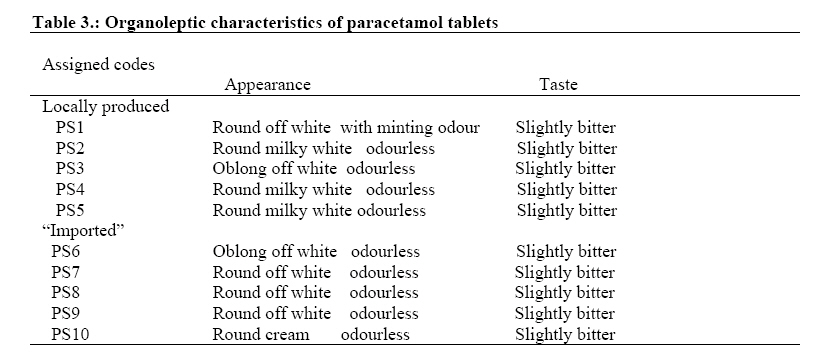
Asaba, Delta State, Nigeria. Code Number: jh07025 SUMMARY Malaria is a major public health problem in endemic countries, and the quality of anti-malarial products is a concern in the therapeutic management of individual patient. In this study, we have evaluated the pharmaceutical quality of chloroquine and paracetamol oral products obtained from a major Nigerian drug “market” using a less elaborate sampling procedure. Results have shown that there are still some defects in the pharmaceutical quality of these drugs, despite the activities of the Nigeria’s drug regulatory agency (National agency for Food and Drug Administration and Control, NAFDAC). 21% (7/34) of the drug products were not registered by NAFDAC. The pharmaceutical properties of the products indicated that 6, 15, 9, and 9% of them failed tests for disintegration, dissolution, crushing strength, and percentage of active content, respectively. 4 out of the 6 chloroquine liquid preparations evaluated had inadequate active content. These defects could have resulted from deliberate counterfeiting, poor quality control during manufacture or decomposition of the products. However, this could not be ascertained from the data available to us in this study. The implication of these findings, however, is that the newer anti-malarial drugs that have recently been introduced into the Nigerian market should be safeguarded, if their therapeutic usefulness must be sustained. Introduction Malaria is one of the most important parasitic diseases in Nigeria and several other tropical and sub-tropical countries of the world. The global burden of the disease stands at 300 – 500 million clinical cases and over a million deaths per year [1]. In addition, huge economic losses are associated with the disease, particularly in sub-Saharan Africa where over 90% of malaria cases are said to occur [2]. In Africa, case management of malaria is one of the most frequently used anti-malarial interventions, despite the documented evidence of other preventive measures such as prevention of the contact between humans and vectors [1]. Until recently, chloroquine was the first line drug in the management of malaria in Nigeria and several other countries where the disease is endemic, because it is cheap and affordable [3]. In addition, chloroquine is often used as anti-malarial prophylaxis for pregnant women, sickle cell anaemic patients and semi-immune and non-immune individuals [3]. Paracetamol is frequently used in addition to chloroquine or other anti-malarial drugs for the management of fever associated with malaria because of its antipyretic activity. However, one of the most important challenges in the chemotherapy of malaria and other infectious diseases in less developed countries, where these diseases are of immense public health importance, is the wide scale availability of fake and substandard drug products [4]. Substandard drugs contribute to the spread of drug-resistant malaria parasites and may lead to increasing therapeutic failure and medical expense [5]. An earlier study by Taylor et al on the pharmacopoeial quality of some essential drugs purchased from two Nigerian urban cities (Lagos and Abuja) showed a high prevalence of substandard products [6]. More than 50% of anti-malarial drugs were found not to have complied with the specifications of British Pharmacopoeia (BP) [6]. The study was undertaken prior to the commencement of efforts by the nation’s National Agency for Food Administration and Control (NAFDAC) to rid the country of fake and substandard products. Nevertheless, to the best of our knowledge, no systematic study has yet assessed the impact of NAFDAC efforts in this regard. We, therefore, undertook this study as part of a proposed large scale study of the quality of anti-malarial drugs in circulation in Nigeria and its implications in achieving global targets of effective malarial intervention in the country. The objective of this study was to evaluate pharmaceutical quality of chloroquine and paracetamol sourced from a major Nigerian drug “market”. Chloroquine and paracetamol were chosen as the study drugs because of their ready availability and use in the country. It has been reported that drug counterfeiting is most commonly associated with “fast moving” pharmaceutical products [7]. Materials and Methods Drug sampling:On a cross-sectional basis, chloroquine and paracetamol tablets (10 brands each) and syrups (6 brands of chloroquine and 8 brands of paracetamol) were purchased in February, 2004 from the market (pharmacies and shops) in Onitsha and a neighbouring town of Asaba, Nigeria, by one of the investigators (JOO) with the assistance of two other persons. The study location was chosen because we envisaged that it may give a better refection of the situation in the country. Drug faking has been linked to “open” drug markets in some major cities in Nigeria, one of which is located in Onitsha. No particular sampling procedure was employed, other than the buyers posing as “normal” customers to purchase the drugs without prescription. The different brands and formulations of the two drugs were sourced from drug stores wherever they were available, until the total number was obtained. Following purchase, information on brand, manufacturer, NAFDAC registration status and expiry date were recorded from the product label. No attempt was made to verify these information. Drug testing:Pharmaceutical properties, including organoleptics (colour, texture, smell and taste), and physicochemical properties (weight, drug content and identification, as well as tablet crushing strength, disintegration and dissolution) were determined. Organoleptic properties were determined (after pulverization in the case of tablets), and examined for colour, texture smell and taste. A panel of six persons who were blinded to source and manufacturer of the drugs carried out the examination, and a majority verdict was taken. Assay of chloroquine and paracetamol contents of the dosage forms were also carried out. Chloroquine was assayed using a validated non-aqueous method [8], while paracetamol was assayed using a validated spectrophotometric method. All procedures, including pH determination, were carried out in duplicate and in accordance with the British Pharmacopoeia 1993 [8]. Results A total of 34 samples of chloroquine and paracetamol phosphate products were analysed. All samples were within shelf life at the time of the study, with an exception of one product (CL14). Twenty one percent (7/34) of the drug products were not registered by NAFDAC. Of these unregistered products, 5 were chloroquine and 2 were paracetamol (Table 1). The organoletic properties indicated that chloroquine and paracetamol tablets were in conformity with BP standards, and did not vary between country of origin (Tables 2 and 3). Results of assessment of the physicochemical properties of the tablet preparations showed that the disintegration of chloroquine tablets ranged from 2.33 minutes to 32.75 minutes, with an average of 6.27 (locally produced) and 15.03 (“imported” products). Two “imported” products, CS6 and CS8 failed the test. Also, there was a tendency for the “imported” products to have high disintegration time as compared to locally produced chloroquine. Percentage dissolution within 45 minutes gave values that ranged from 45.51 to 104.30, with only one product, CS6 having percentage dissolution in 45 minutes of less than the 70% minimum stipulated by the BP. The content of chloroquine tablets was found to be within normal range, except for one imported product, CS6, which had a percentage of the stated amount of 116.5%, a value outside the BP range of 92.5 – 107.5% (Table 4). The disintegration time for all paracetamol tablets were within the pharmacopoeial range (≤15 min), while percentage tablet dissolution of the drug in 45 minutes ranged from 64.26 to 73.06, with four products (PS 3, 4, 5 and 7) failing the test. In terms of percentage of stated amount, two products, PS1 and PS8, were found to be outside the pharmacopoeial range (95 to 105%) for paracetamol (Table 5). There is no pharmacopoeial requirement for tablet crushing strength, but in industrial practice, 4kg is generally considered a minimum. The crushing strengths for chloroquine and paracetamol tablets were found to be within 7.34 to 13.32 kg and 1.91 to 7.28kg, respectively. Three chloroquine products, (all locally produced, CS1, CS2 and CS3) did not conform to the requirement. Table 1: Description of chloroquine and paracetamol tested for pharmaceutical properties.
All liquid preparations of chloroquine and paracetamol were packaged in amber colour bottle with an exception of one, CL15, which was packaged in a white 2L container. Other pharmaceutical properties of chloroquine and paracetamol liquid preparations are shown in Tables 6 and 7. None of the chloroquine syrups and only three paracetamol syrup products (PL11, 12 and 13) met the BP requirements for pH. Discussion Traditionally, the problem of counterfeit pharmaceuticals has been limited to developing nations in Asia and Africa. Now, drug counterfeiting is rapidly becoming a worldwide concern, and counterfeit drugs are beginning to reach the advanced markets [9].Though artemisinin-based combination drugs have been officially adopted by the Federal Government of Nigeria as the first line anti-malarial drugs, a majority of health care providers and consumers in the country still prefer to use chloroquine because it is very affordable. They contend that the real problem with chloroquine chemotherapy is the widespread faking of the product resulting in suboptimal therapeutic response. Table 2: Organoleptic characteristics of chloroquine tablets
Table 4: Physicochemical characteristics of chloroquine tablets
DT = disintegration time, D45mins
= percentage dissolution in 45 minutes, W = average weight per tablet, Table 5: Physicochemical characteristics of paracetamol tablets
DT = disintegration time, D45mins = percentage dissolution in 45 minutes, W = average weight per tablet, DC = drug content, PA = percentage of label strength While it may be understood that counterfeit anti-malarial drugs pose a great threat to the lives of patients with malaria [10], it has not be possible to consistently evaluate the prevalence of substandard drugs in circulation, especially in the less developed countries. Also, in spite of the fact that international organisations such as the World Health Organization, have devised specific measures to combat counterfeit trade, the problem still remains quite daunting. Furthermore, although the practice of drug counterfeiting is unlikely to ever completely disappear, it may be controlled if governments and all relevant parties combine forces to identify and disrupt the counterfeit chain [11].Poor quality of medicinal products could result from poor quality control of drugs during manufacture, chemical instability due to hot climatic condition and outright faking of medicines [6]. This study evaluated NAFDAC registration status, product stocking beyond expiration date, organoleptic and physicochemical properties of two products, which were sourced from the Nigerian market, and are important in the chemotherapy of malaria. Physicochemical properties are important considerations in solid dosage form. For example, disintegration measures the time required for tablets to disintegrate into particles prior to dissolution. British Pharmacopoeia (1993) [8] stipulates a time of not more than 15 minutes (uncoated tablets) and 30 minutes (capsules). The results showed that all paracetamol products tested passed the requirement, while two “imported” brands of chloroquine failed to meet the specification. Dissolution on the other hand measures the release characteristics of active ingredients in vitro from solid dosage form. It gives a fair indication of drug absorption into the systemic circulation in order to exert its pharmacologic and clinical effects. The BP (1993) specifies that at 45 minutes all tablets and capsules should release an amount not less than 70% of the label claim into the dissolution medium. Four paracetamol products and one chloroquine product, CS6, failed to meet the specification. Poor formulation, especially the type and/or quantity of excipients may affect disintegration and dissolution characteristics of solid dosage form. However, this was not investigated in this study. The crushing strength of tablets measures its ability to resist chipping, abrasion or breakage during storage, transportation and handling. Failure in crushing strength of pharmaceutical solid dosage form could result from inadequate binding agent during formulation or insufficient compression during tableting. Findings from this study indicate that 85% of the solid dosage forms passed the test; the products that failed the test were locally produced. The Pharmaceutical Codex [12] stipulates that for maximum stability, the pH of liquid chloroquine and paracetamol preparations should be within 4.2 to 5.0 and 5 to 7, respectively. The results show that none of the liquid chloroquine preparations passed the test, while only 50% of the liquid paracetamol products conform to the specification (Table 6). Furthermore, 4 out of the 6 chloroquine liquid preparations evaluated had inadequate active content. In fact, no active ingredient was found in one of the products, CL15 (Table 7). The implication of this is that when such products are given, the patient might fail to show adequate clinical response. Table 6: Organoleptic characteristics of chloroquine and paracetamol liquid preparations
Table 7: Physicochemical characteristics of chloroquine and paracetamol liquid products
LS = label strength, *are imported liquid paracetamol products Conclusion Despite the concerted efforts by NAFDAC in ensuring that safe and effective drugs are in circulation in the country, this study has shown that there are still some defects in the pharmaceutical quality of chloroquine and paracetamol sold in Nigeria. A number of the products fell below the regulatory standards irrespective of the country of origin. Whether these defects result from deliberate counterfeiting, poor quality control during manufacture or decomposition of the products could not be ascertained. However, findings from the study serve as signals for newer anti-malarial drugs (e.g. artemisinin-based combination drugs) that were recently introduced into the Nigerian market. It is important that these products are safeguarded in order to prolong their therapeutic usefulness. Availability of safe and effective anti-malarial drugs is one strategy aimed at attaining the United Nations’ malaria-related Millennium Development Goals. References
© Copyright 2007 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh07025t1.jpg] |
| |||||||||

{kind=link}